Discharge, Itching, Odor: Yeast Infection or Bacterial Vaginosis?
When a patient tells me, “Doctor, I think I have another yeast infection,” I’m always a bit cautious. Not because she’s necessarily wrong, but because in practice, intimate symptoms can easily mimic one another.
Throughout the years, from my training at Cerrahpaşa to my time in Franche-Comté and over +30 years of practice in gynecology and reproductive medicine, I’ve seen this confusion hundreds of times. One woman treats a yeast infection… when it’s actually BV. Another thinks she has an infection… when she’s simply reacting to an irritant. A third ends up believing she has “something serious,” when it’s a common but misidentified issue.
The real goal isn’t just to relieve quickly—it’s to relieve correctly.
🎥 Video by Dr. Senai Aksoy
📌 What You Will Learn in This Article
- How to tell the difference between a yeast infection and BV?
- What symptoms point toward a vaginal yeast infection?
- Which signs suggest bacterial vaginosis?
- Why is odor often an important clue?
- What other causes can mimic a yeast infection or BV?
- In which cases should you consult a doctor quickly?
- How is the diagnosis confirmed in the clinic?
- How to limit recurrences?
How to tell the difference between a yeast infection and BV?
If I had to summarize it simply, I would say this: yeast infections irritate more, BV smells more. It’s a useful rule of thumb, but not a mathematical law. In consultation, we piece together several clues: the appearance of the discharge, the odor, the intensity of itching, the context, the vaginal pH, and sometimes a microscopic examination.
Thick white discharge with significant itching points more toward vulvovaginal candidiasis, while malodorous thin discharge suggests bacterial vaginosis, as reminded by the MSD Manual on Vaginitis and the CDC Recommendations on BV.
If you are on a fertility journey, you can also read our article on female infertility in the context of IVF treatments as well as our dossier on hydrosalpinx and its impact on fertility.
What symptoms point toward a vaginal yeast infection?
A vaginal yeast infection, in its classic form, is primarily a story of irritation. Patients often tell me: “it burns,” “it itches intensely,” “I feel like everything is irritated.” The discharge is often thick, whitish, and sometimes frankly clumpy.
What mainly points to vulvovaginal candidiasis is:
- Marked pruritus (itching);
- A burning sensation;
- Vulvar redness;
- Sometimes slight swelling;
- Thick white discharge;
- Discomfort during intercourse or urination in some cases.
What many forget is that a yeast infection doesn’t necessarily produce a strong foul odor. When odor clearly dominates the picture, I start looking elsewhere.
Which signs suggest bacterial vaginosis?
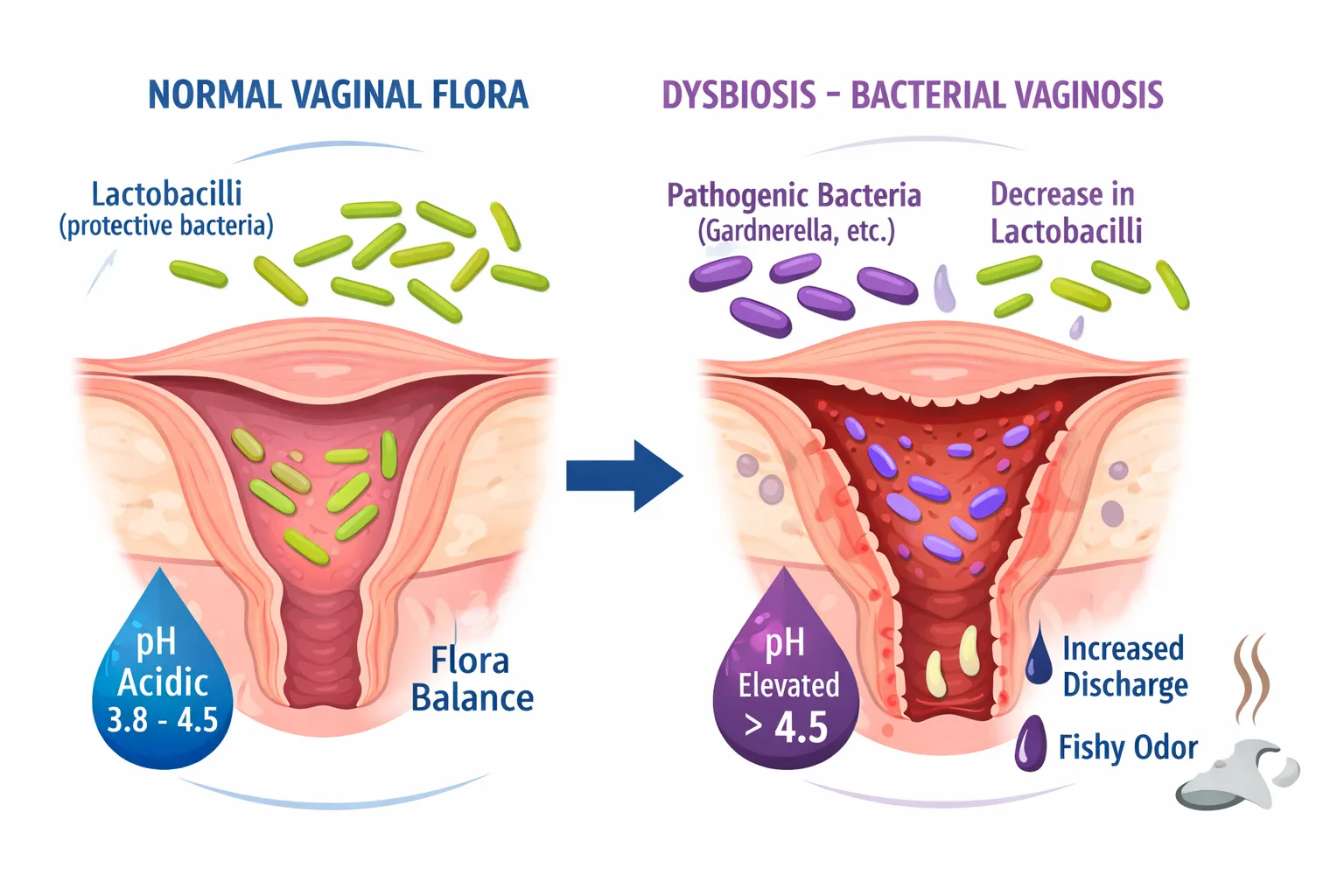
Bacterial vaginosis is not, in the clinician’s mind, just another “vaginal infection.” It is rather an imbalance of the vaginal ecosystem. Lactobacilli, which normally play a protective role, become fewer in number. The pH rises. Other bacteria take their place.
That’s when symptoms appear, often with a very specific logic: less itching than a yeast infection, but more thin discharge and especially that famous fishy odor, caused by the release of amines by anaerobic bacteria like Gardnerella vaginalis or Mobiluncus.
The signs suggesting BV are often:
- Thin, grayish, and homogeneous discharge;
- A more distinct intimate odor (often a positive “whiff test” in the clinic);
- A vaginal pH higher than 4.5;
- An unbalanced flora (disappearance of protective lactobacilli);
- Little to no pruritus (itching).
In practice, it’s often the odor that catches our attention long before anything else.
Why is odor often an important clue?
Because it provides real clinical information. Not always sufficient, but often very diagnostic.
Many women hesitate to talk about it out of embarrassment. That’s a shame, because this detail is sometimes the most useful element of the entire consultation. A fishy odor, especially if it accompanies thinner discharge, makes me think primarily of bacterial vaginosis.
Conversely, a pure yeast infection can be very uncomfortable without significantly changing the odor. In other words: in gynecology, odor isn’t an embarrassing detail—it’s often a valuable diagnostic clue.
What other causes can mimic a yeast infection or BV?
This is probably one of the most important points in this article. Not everything that itches is a yeast infection. Not everything that leaks is BV. And not everything that feels uncomfortable is infectious.
In real life, many intimate symptoms are related to something else: a harsh soap, intimate perfume, panty liners, friction, dryness related to menopause, vulvar dermatosis, or even a forgotten tampon. The MSD Manual on Vaginitis reminds us that a significant portion of vulvovaginitis cases are non-infectious.

Among the causes that can mimic an infection, we often find:
- Soaps, gels, or scented products;
- Lubricants or spermicides;
- Tight clothing or synthetic underwear;
- Hypoestrogenism of menopause;
- Certain dermatoses like eczema or lichen;
- A forgotten foreign body;
- Certain STIs like trichomoniasis.
This is where self-diagnosis errors begin. The patient treats a “yeast infection” that isn’t one. Then she concludes that “nothing works.” In reality, it’s not that the treatment is bad—it simply isn’t targeting the right problem.
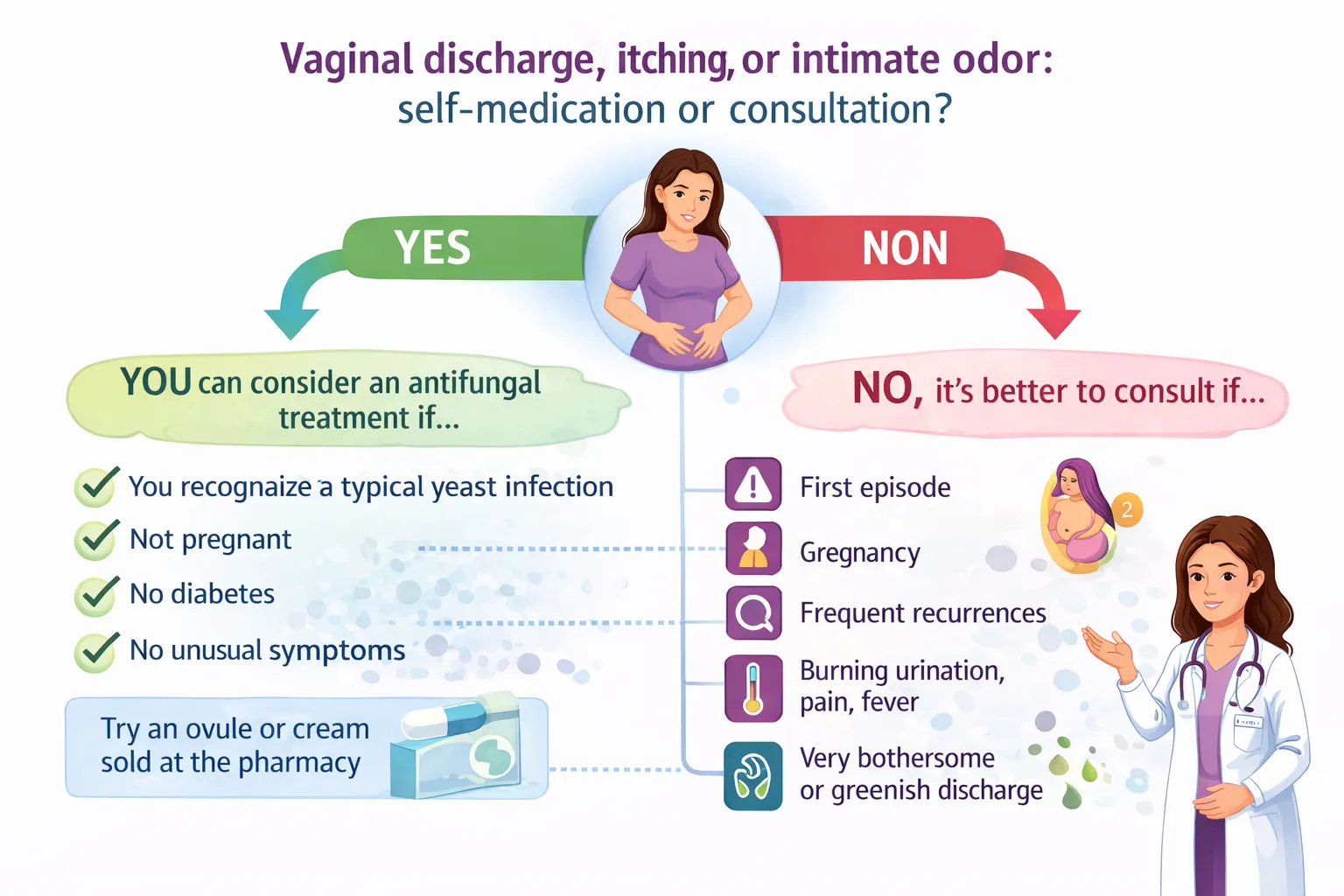
In which cases should you consult a doctor quickly?
You should consult when the situation doesn’t resemble a simple, already known, and easily recognizable episode. The first episode often deserves a real diagnosis. Pregnancy also changes the situation. Pelvic pain, fever, significant urinary burning, frankly greenish discharge, or a lack of improvement are also signals that should prompt a consultation.
The CDC recommendations on vulvovaginal candidiasis also insist on caution in cases of recurrence, diagnostic doubt, or an atypical presentation.
How is the diagnosis confirmed in the clinic?
This is where medicine becomes concrete. We listen to the symptoms, of course, but we don’t stop there. We examine. We look at the aspect of the discharge. We can measure the pH. Depending on the context, we complete with a microscopic exam or a swab.
The MSD Manual on Vaginitis describes this approach well.
For bacterial vaginosis, we often look for:
- Suggestive discharge;
- A pH greater than 4.5;
- An amine odor;
- Clue cells.
For a yeast infection, we more commonly find:
- A compatible clinical picture;
- A pH that is often normal or low;
- Yeasts or pseudohyphae.
Sometimes it’s very simple. Sometimes much less so. But in all cases, it’s these details that prevent treating an irritation like an infection, or BV like candidiasis.
How is a vaginal yeast infection treated?
A simple vulvovaginal yeast infection is generally treated with a local antifungal, and sometimes orally depending on the case. But not all yeast infections are the same. When episodes recur, when the usual treatment no longer works, or when the presentation becomes atypical, the strategy must be reviewed.
The CDC recommendations on vulvovaginal candidiasis very clearly distinguish simple episodes from recurrent, severe, or non-albicans forms.
How is bacterial vaginosis treated?
Bacterial vaginosis is most often treated with metronidazole or clindamycin, depending on the situation. The reference therapeutic regimens are detailed in the CDC recommendations on bacterial vaginosis.
This is where self-medication shows its limits. Many women take an antifungal treatment because they spontaneously think of a yeast infection. If the cause is bacterial, this treatment logically has no reason to work.
Why does it sometimes return after antibiotics, periods, or intercourse?
Because the vagina functions as a literal ecosystem. When this balance is disrupted, certain yeasts or opportunistic bacteria take advantage of the situation. Recent antibiotic therapy can favor candidiasis. Other factors, such as vaginal douching or certain local changes, can favor dysbiosis.
This logic is well explained in this PubMed review on the pathophysiologic interrelationship between bacterial vaginosis and candidiasis.
The most frequent contributing factors include:
- Recent antibiotic therapy;
- Vaginal douching;
- A weakened microbiota;
- Irritating products;
- Recurrences treated without re-checking the diagnosis.
How to limit recurrences?
Prevention often rests on very simple things, but they must be done regularly: gentle intimate washing without excess; no vaginal douching; breathable underwear; caution with scented products; and especially re-evaluation if symptoms change or return too often.
The CDC on bacterial vaginosis also reminds us that vaginal douching can favor relapses.
🛑 Home Remedies vs. Medical Reality
You often read on the internet that applying yogurt, garlic, or coconut oil can “cure” a yeast infection or BV. As a doctor, I want to be clear: these methods are not scientifically validated. Worse, they can worsen irritation or introduce new bacteria into an already fragile ecosystem. The balance of the vaginal microbiota is complex; only a targeted treatment (antifungal or antibiotic) can safely restore intimate health.
👥 Should the partner be treated?
This is a very frequent question in consultation.
- For a yeast infection: Treatment of the partner is generally not necessary unless he has symptoms himself (redness, irritation of the glans). A yeast infection is not considered an STI (Sexually Transmitted Infection).
- For BV: Current studies and ACOG (American College of Obstetricians and Gynecologists) or RCOG guidelines do not indicate routine treatment of the male partner, as it does not reduce the risk of recurrence in the woman.
- In case of persistent recurrences: A broader discussion on couple habits and respecting flora balance can be helpful.
What is the link with fertility, pregnancy, and IVF?
A simple yeast infection, on its own, generally has no major consequence on fertility. However, recurrent symptoms, poorly identified issues, or those associated with other pelvic problems must be evaluated seriously, especially in a context of desiring pregnancy or undergoing IVF.
See Also
If you would like to learn more about fertility and reproductive health topics, feel free to consult our dedicated resources:
- Female Infertility in IVF Treatments
- Hydrosalpinx and Its Consequences on Fertility
- Our page dedicated to IVF / ICSI Fertilization.
FAQ — Frequently Asked Questions
Does a fishy odor always mean bacterial vaginosis?
Not necessarily, but it is a very suggestive sign. When this odor is associated with thin discharge, BV becomes a strong hypothesis.
Can you have itching with BV?
Yes, it is possible. But generally, in BV, the odor and discharge modifications are more characteristic than pruritus.
Is thick white discharge typical of a yeast infection?
Yes, especially if accompanied by itching and burning.
Can I treat myself with an antifungal suppository?
Only if you recognize a known yeast infection very well, in a simple context, without pregnancy or unusual signs.
Is bacterial vaginosis an STI?
Strictly speaking, in most cases, it is not. It is mainly a dysbiosis. However, other sexually transmitted infections can produce similar symptoms.
Why does it often return after antibiotics?
Because certain antibiotics disrupt the protective vaginal flora, which can favor secondary candidiasis.
Can you have a yeast infection and BV at the same time?
Yes, it can happen. Some patients even experience successive or mixed episodes on a fragile flora background.
When should you consult as a relative priority?
In case of pregnancy, pain, fever, significant urinary burning, greenish discharge, recurrences, or lack of improvement.
Medical References
- CDC — Bacterial Vaginosis: STI Treatment Guidelines
- CDC — Vulvovaginal Candidiasis: STI Treatment Guidelines
- MSD Manual — Overview of Vaginitis
- ACOG — Vaginitis in Nonpregnant Patients
- PubMed — Bacterial Vaginosis and Vulvovaginal Candidiasis Pathophysiologic Interrelationship
Legal Disclaimer
Date of last medical review: March 13, 2026.
This article was written and medically validated by Dr. Senai Aksoy (Gynecologist-Obstetrician, Specialist in Reproductive Medicine) for strictly informative purposes. Every patient is unique and gynecological symptoms can have several causes. This content in no way replaces a medical consultation, a clinical exam, or a vaginal swab when necessary. Please always consult your doctor regarding your personal situation.
© Assoc. Prof. Dr. Senai Aksoy - All rights reserved.

The content has been created by Dr. Senai Aksoy and medically approved.