Vaginitis and Vaginal Flora: What Is Normal and When It Is Not
Key Takeaways
Normal vaginal flora is usually dominated by protective lactobacilli and a low vaginal pH. Vaginitis happens when that balance changes or when infection is present, and the right treatment depends on identifying whether the cause is bacterial vaginosis, yeast, trichomoniasis, irritation, or low-estrogen change rather than guessing from symptoms alone.
Key evidence: CDC bacterial vaginosis treatment guidelines Liu et al. 2025 — bacterial vaginosis and microbial dysbiosis review
On this page
- What normal vaginal flora does
- What vaginitis means
- Common causes
- Why testing matters
- What “shift in vaginal flora” or a Gardnerella result means
- Treatment depends on the diagnosis
- Conclusion
Vaginitis and Vaginal Flora: What Is Normal and When It Is Not
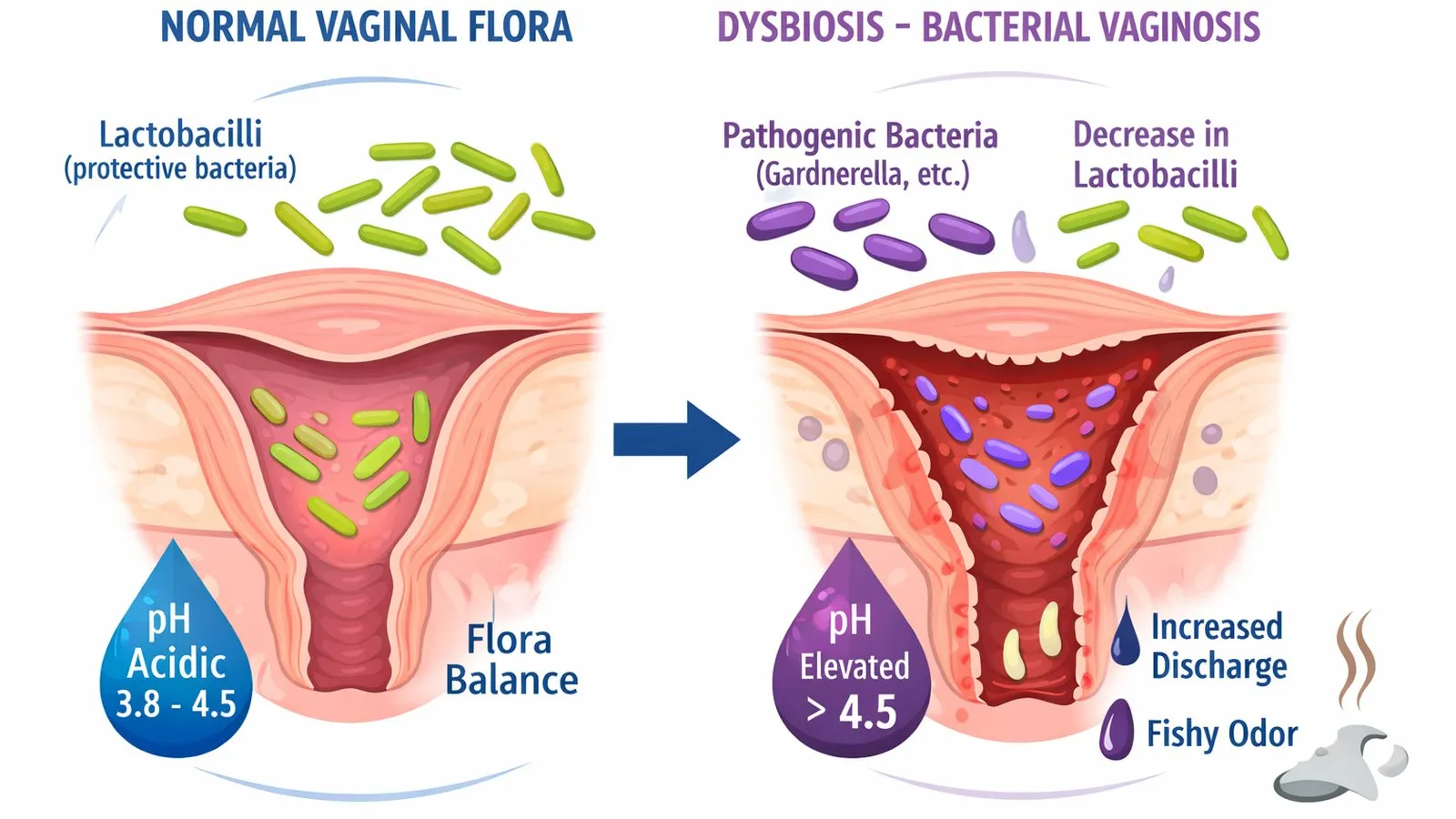
The vagina normally hosts a complex, balanced microbial environment. In reproductive-age patients, lactobacilli typically keep the pH acidic and create conditions that limit overgrowth of less favorable organisms. Symptoms tend to appear once that balance shifts, or once infection or irritation sets in.
What Normal Vaginal Flora Does
The healthy vaginal environment is maintained by protective Lactobacillus species.
Functions of normal vaginal flora:
- Acidic Environment: Maintains a low vaginal pH (3.8–4.5) through lactic acid production.
- Pathogen Inhibition: Produces hydrogen peroxide ($H_2O_2$) and bacteriocins to inhibit pathogenic growth.
- Dynamic Balance: Fluctuates naturally with menstrual cycles, sexual activity, antibiotics, and hormonal shifts.
What Vaginitis Means
Vaginitis refers to mucosal inflammation or dysbiosis characterized by:
- Abnormal vaginal discharge (altered color, consistency, or volume).
- Vulvovaginal itching, burning, or redness.
- Malodor (often described as fishy in bacterial vaginosis).
- Dyspareunia (painful intercourse) or dysuria.
Common Causes
- Bacterial Vaginosis (BV): Shift from Lactobacillus to anaerobic overgrowth (Gardnerella, Atopobium). Elevated pH (> 4.5).
- Vulvovaginal Candidiasis (Yeast): Candida albicans fungal overgrowth. Normal pH (3.8–4.5), thick curd-like discharge, intense pruritus.
- Trichomoniasis: Trichomonas vaginalis protozoan STI. Frothy yellow-green discharge, elevated pH.
- Atrophic Vaginitis: Estrogen deficiency leading to mucosal thinning and dryness (postmenopausal or postpartum).
Why Testing Matters
Symptom overlap is frequent. Microscopic examination (wet mount, KOH prep), pH indicator testing, and nucleic acid amplification tests (NAAT) are required for accurate diagnosis before initiating antimicrobial therapy.
What “Shift in Vaginal Flora” or a Gardnerella Result Means
A lab report indicating “shift in flora” or “Gardnerella detected” is not an automatic indication for antibiotic treatment.
Key clinical considerations:
- Gardnerella vaginalis can be present in up to 30–40% of healthy, asymptomatic women (Troha et al. 2026).
- Amsel Criteria & Nugent Score: Diagnosis requires clinical signs (discharge, positive whiff test, clue cells, pH > 4.5) alongside lab markers (Liu et al. 2025).
- Partner Treatment: Routine male partner treatment is not recommended for BV or yeast infections, but is mandatory for trichomoniasis.
Dr. Aksoy’s Clinical Perspective:
“Finding Gardnerella on a lab report does not mean an STI or an automatic prescription for antibiotics. We treat the patient’s clinical symptoms and exam findings—not isolated lab reports.”
Treatment Depends on the Diagnosis
- Bacterial Vaginosis: Metronidazole or clindamycin (oral or intravaginal).
- Yeast Infection: Azole antifungals (fluconazole oral or intravaginal suppositories).
- Trichomoniasis: Oral metronidazole or tinidazole (simultaneous partner treatment required).
- Atrophic Vaginitis: Local topical vaginal estrogen therapy.
Conclusion
It helps to think of vaginitis less as a single infection and more as a symptom pattern with several possible causes. Normal flora is the backdrop that explains why pH, lactobacilli, hormones, and targeted testing all matter when choosing the right treatment.
Request a Case Review
If your discharge, odor, or irritation doesn’t fit a clear pattern — or a lab report used language like “shift in flora” without a plain explanation — a targeted examination and testing is more useful than guessing from symptoms alone. You can request a confidential case review if you’d like a second opinion on a result you’ve already received.
Related Reading
- Twin Pregnancy After IVF: Why One Embryo Is Often the Safer Plan
- Discharge, Itching, Odor: Yeast Infection or Bacterial Vaginosis?
- Vaginal Microbiome and IVF: What Lactobacillus Dominance May Mean for Implantation
FAQ
Can symptoms alone tell the cause of vaginitis?
Not reliably. Odor, itching, discharge, and irritation can overlap across bacterial vaginosis, yeast infection, trichomoniasis, irritation, and low-estrogen changes.
Is bacterial vaginosis the same as a yeast infection?
No. Bacterial vaginosis is linked to a shift away from lactobacillus-dominant flora, while yeast infection is usually caused by Candida overgrowth — and each is treated differently.
Does every vaginitis diagnosis require partner treatment?
No. Partner treatment depends on the diagnosis. Trichomoniasis requires sexual partner management, while bacterial vaginosis and yeast infection are handled differently.
Why does vaginal pH matter?
Vaginal pH helps guide diagnosis because bacterial vaginosis and trichomoniasis often raise pH, while uncomplicated yeast infection may occur with a normal pH.
Sources
- Centers for Disease Control and Prevention. Vulvovaginal - STI treatment guidelines.
- Centers for Disease Control and Prevention. Bacterial vaginosis - STI treatment guidelines.
- MedlinePlus. Vaginitis.
- Liu D, Zhang X, Zhao X, Che X, Song W, Wu G. Bacterial vaginosis: advancing insights into microbial dysbiosis. Crit Rev Microbiol 2025;52(1):159-175.
- Troha N, Zorec TM, Hošnjak L, et al. Bacterial microbiome analysis of vaginal, cervical, and endometrial samples in patients with adenomyosis during the window of implantation. Microbiol Spectr 2026;14(4):e0279125.
Add as a Preferred Source on Google
You can add draksoyivf.com as one of your preferred health information sources on Google.

The content has been created by Dr. Senai Aksoy and medically approved.