Does Endometriosis Show Up on Ultrasound? A Guide to Ultrasound, MRI and Laparoscopy
Key Takeaways
Yes — some forms of endometriosis can be seen on ultrasound, especially ovarian endometriomas and many deep lesions, when an experienced operator uses the four-step IDEA protocol. Superficial peritoneal disease may still be missed, so a normal scan does not rule the condition out. MRI helps when ultrasound is inconclusive. CA-125 is not for screening or routine monitoring. Laparoscopy is no longer an automatic first step under ESHRE 2022 and NICE 2024.
Key evidence: ESHRE guideline: endometriosis (2022) NICE NG73 — endometriosis diagnosis (updated 2024) IDEA protocol — Guerriero et al., 2016
Does endometriosis show up on ultrasound?
Yes — some forms can. Ovarian endometriomas and many deep lesions often show up when an experienced operator follows a structured scan. Superficial peritoneal endometriosis may not appear at all. So a normal ultrasound does not close the case.
For years, laparoscopy was treated as the only way to “prove” endometriosis. Waiting for surgery before recognising the diagnosis may have added to delay — along with symptoms being dismissed as “normal periods,” late referral, and limited access to specialist imaging. Diagnostic delay remains common, and it varies widely by country and health system.
The ESHRE 2022 guideline put imaging first and kept laparoscopy for situations where it would change care. The goal is practical: shorten delay, avoid operations that do not help, and start symptom-led care earlier when the picture fits — while recognising that a woman whose priority is pregnancy needs a different path from one whose priority is pain control.
This page walks through the modern toolkit. For the wider picture, see the complete endometriosis guide, endometriosis and infertility, and endometriosis symptoms.
Diagnosis starts before the scan: symptoms and examination
Imaging does not replace listening — or examining.
Clues that raise suspicion include period pain that gets worse over time, deep pain with intercourse, cyclic bowel pain or painful bowel movements, cyclic urinary pain or blood in the urine, chronic pelvic pain, infertility, a family history, fatigue, and a clear impact on school, work, intimacy or daily life. Previous surgery and how painkillers or hormonal treatment have helped (or not) also matter.
On examination, a uterus that moves poorly or sits fixed in retroversion, tenderness or nodularity in the posterior fornix, tender uterosacral ligaments, or an adnexal mass can support the suspicion. A normal pelvic examination does not exclude endometriosis, especially early or superficial disease. NICE still recommends offering ultrasound when endometriosis is suspected, even if the examination feels normal.
When to seek prompt assessment
Do not wait for a routine endometriosis pathway if you have sudden severe pain on one side; fainting or marked dizziness; pain or bleeding with a positive pregnancy test; fever; heavy bleeding with fainting, marked dizziness, weakness or a rapid heartbeat; a rapidly enlarging or unusual ovarian mass; new postmenopausal pelvic pain or a new mass; symptoms of bowel obstruction; frank blood in the urine; or concern that a ureter is blocked and the kidney is becoming swollen (hydronephrosis). These need prompt assessment.
Transvaginal ultrasound following the IDEA protocol
The IDEA protocol (International Deep Endometriosis Analysis), published by Guerriero et al. in 2016, turns a free-form pelvic scan into four clear steps. The same findings can also be described with mapping systems such as #Enzian, which helps teams speak a shared language about where disease sits.
If a vaginal scan is not appropriate or acceptable — including for adolescents and anyone who declines vaginal examination — transabdominal ultrasound can come first. Specialist MRI, or in selected settings a transrectal scan, may follow according to symptoms, the suspected site of disease and preference.
Step 1 — uterus and adnexa
The operator looks at:
- how freely the uterus moves, and whether it is fixed in retroversion;
- signs of adenomyosis (asymmetric wall thickening, tiny myometrial cysts, subendometrial lines or buds);
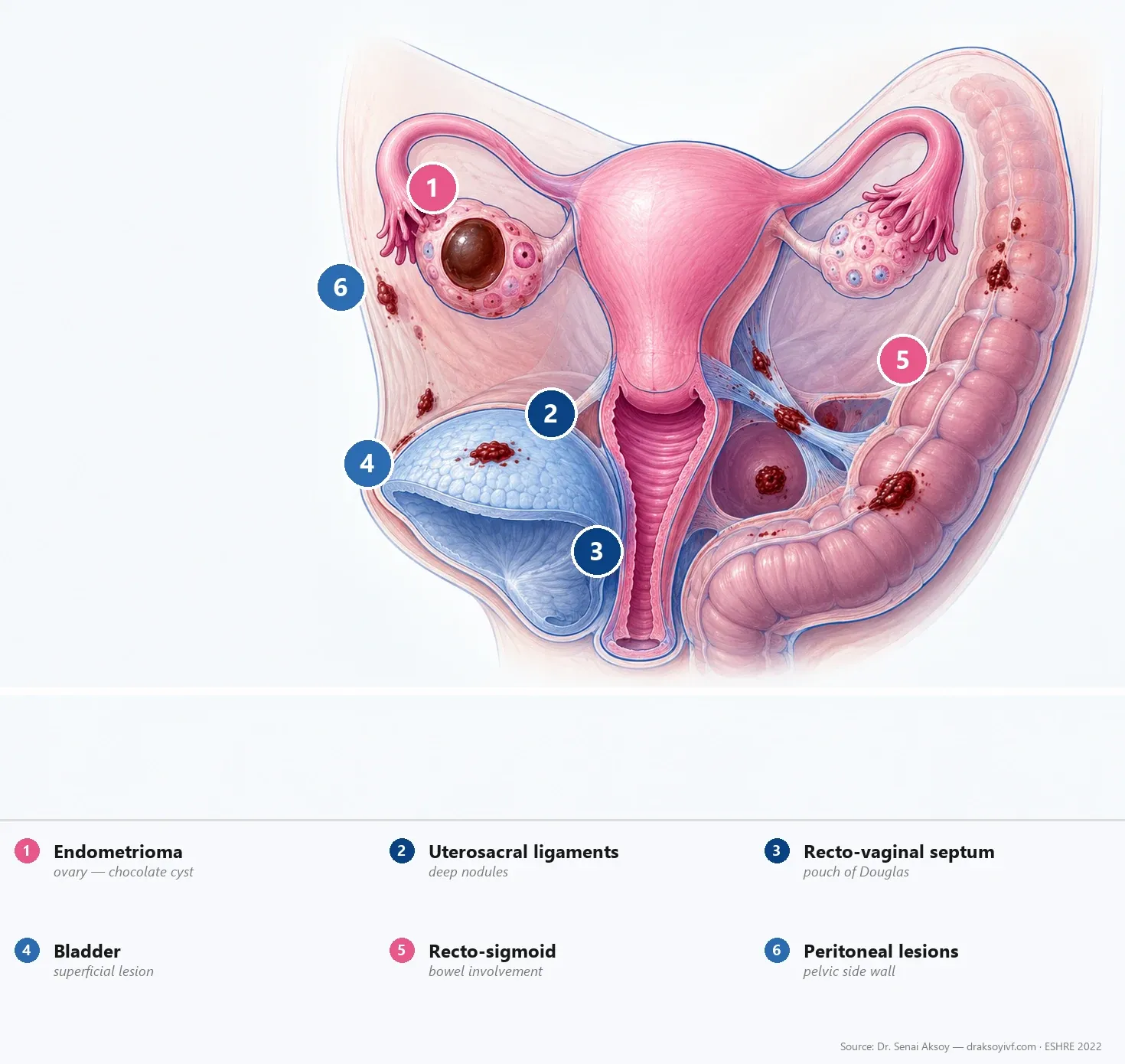
- ovarian cysts — size, texture, blood flow — with special care for an endometrioma—sometimes called a “chocolate cyst”—which often has a homogeneous “ground-glass” appearance on ultrasound;
- when fertility matters, an antral follicle count may be recorded too. It is not a diagnostic test for endometriosis.
Finding an endometrioma does not mean it must be removed. Before any surgical decision, age, symptoms, AMH, follicle count, previous ovarian surgery, whether both ovaries are involved, and IVF plans should be reviewed together.
Step 2 — soft markers
Two indirect signs are checked:
- Ovarian tenderness when the probe presses — may support local pelvic disease, but it is not specific to endometriosis.
- Ovarian fixation — the ovary does not slide freely against the pelvic wall or uterus, which can suggest adhesions.
Step 3 — sliding sign
Gentle pressure on the abdomen shows whether the uterus glides over the rectum in the Pouch of Douglas.
- Positive sliding sign: free movement makes obliteration of the Pouch of Douglas less likely. It does not rule out adhesions elsewhere in the pelvis.
- Negative sliding sign: restricted movement suggests partial or complete obliteration of the pouch, often linked with posterior deep endometriosis.
Step 4 — anterior and posterior compartments
A systematic search for deep nodules:
- Anterior: bladder wall, vesico-uterine pouch.
- Posterior: uterosacral ligaments, rectovaginal septum, rectal and sigmoid wall, vagina.
Deep nodules usually look hypoechoic, irregular and poorly defined, sometimes with small cystic spaces. Mapping helps estimate extent, guide referral and plan treatment. If surgery is needed, it also helps assemble the right team. Operations involving bowel, bladder or ureters belong in an experienced multidisciplinary setting.
Diagnostic performance
In experienced hands, transvaginal ultrasound is highly accurate for ovarian endometriomas, and expert scanning is also highly accurate for rectosigmoid deep endometriosis. Accuracy for other deep sites still varies by location and by who holds the probe. Superficial peritoneal disease remains the main blind spot: lesions are often too small or subtle for reliable detection on ultrasound or MRI. Normal imaging cannot exclude them.
An IDEA scan by someone untrained in the protocol can underestimate disease. Experience matters.
Pelvic MRI: when and why
MRI helps when:
- ultrasound is inconclusive and symptoms remain strong;
- deep disease needs detailed mapping of rectum, sigmoid, ureters, bladder and the other pelvic compartments. Suspected diaphragmatic or thoracic endometriosis needs a dedicated upper-abdominal or chest protocol — a standard pelvic MRI does not routinely cover the diaphragm;
- clinical findings and ultrasound disagree;
- a vaginal scan is not appropriate, alongside transabdominal ultrasound and specialist referral.
Typical sequences look for old blood that endometriosis leaves behind. Vaginal or rectal gel is used in some centres and not in others; it is not required in every protocol.
Specialist MRI and expert ultrasound can both map deep disease well. Which performs better depends on lesion site, protocol and expertise. They work best as partners, not as rivals. MRI is also limited for superficial peritoneal lesions.
CA-125: not for screening or routine monitoring
CA-125 is a blood tumour marker that can rise in endometriosis — and in many unrelated situations: a normal period, a functional ovarian cyst, pelvic infection, fibroids, ovarian cancer, pregnancy, ascites or peritonitis. Its sensitivity is particularly poor early in disease.
ESHRE 2022 advises against using biomarkers such as CA-125 to screen an asymptomatic woman, or to confirm or rule out endometriosis in someone with symptoms.
It has no routine role in monitoring disease activity or treatment response. It may occasionally sit inside a broader work-up of an atypical ovarian mass when cancer is also on the list — but never alone, and it cannot tell endometriosis from ovarian malignancy by itself.
The new place of laparoscopy
Guidelines agree on one shift: laparoscopy should no longer be the automatic first step. ESHRE no longer treats it as the default gold standard. It is usually considered when imaging is negative but symptoms remain strongly suggestive, or when empirical treatment has failed, is unsuitable, or is not acceptable. NICE 2024 notes the same point: laparoscopy may still be considered when ultrasound or MRI is normal but clinical suspicion persists. The real question is whether surgery would change management — given symptoms, treatment goals and fertility plans.
When laparoscopy is still considered
- Negative imaging in a symptomatic woman whose pain is not controlled, or for whom hormonal empirical treatment is unsuitable.
- A clear therapeutic need: removing painful lesions, freeing adhesions, treating deep disease involving bowel or urinary tract.
- Selected infertility situations — see below.
- Suspected associated pathology that imaging has not clarified.
What laparoscopy should no longer be
- A mandatory step before any medical treatment.
- A screening tool in an asymptomatic woman with “clinical doubt.”
- A reflex response to pelvic pain before goals and options have been properly reviewed.
When laparoscopy is done, suspicious lesions should usually be biopsied. A negative biopsy does not completely exclude endometriosis if sampling was limited or not representative.
Empirical treatment: for pain — not while trying to conceive
If the clinical picture is suggestive and initial imaging is reassuring (no endometrioma, no deep disease, no suspicious mass), empirical symptom treatment may include analgesics and, when appropriate, a continuous combined hormonal contraceptive or a progestogen — for someone whose immediate priority is pain control and who is not trying to conceive.
If pregnancy is the goal: hormonal empirical treatment is for symptoms, not fertility. It is not appropriate while actively trying to conceive, and it does not improve the chance of pregnancy. Age, ovarian reserve, tubal status, semen analysis, how long infertility has lasted, and the possible role of surgery or IVF should be assessed without unnecessary delay.
Response should be reviewed after an individually agreed period — not after a fixed universal interval. Persistent or worsening symptoms, poor tolerance, fertility priorities, or suspected bowel, bladder or ureteric disease may justify earlier specialist imaging or surgical discussion. If hormonal treatment is unsuitable because pregnancy is desired, the pathway should shift toward fertility assessment rather than suppression.
Does suspected endometriosis change the infertility work-up?
AMH and antral follicle count do not diagnose endometriosis. They help with fertility planning and with estimating the ovarian cost of surgery. Tubal assessment should not be skipped when relevant. Semen analysis should not wait. Hormonal suppression is not a fertility treatment.
Laparoscopy is not a routine test for every woman with a normal scan and open tubes. The decision turns on age, ovarian reserve, pain, previous surgery, duration of infertility, semen analysis, tubal findings, other infertility factors, and whether spontaneous conception or IVF is the realistic next step. ESHRE frames surgical decisions the same way — around those factors and preference, not around producing a label.
My approach when someone is trying to conceive: I do not recommend laparoscopy simply to “prove” endometriosis. I ask first whether the finding would change the route to pregnancy. In a younger woman with good ovarian reserve, open tubes and no major male factor — especially if pain is also significant — surgery may occasionally support a period of spontaneous conception. In an older woman, or one with low reserve, bilateral endometriomas or other clear IVF indications, diagnostic surgery can cost valuable time and sometimes reduce ovarian reserve further. The decision should serve the pregnancy plan, not merely the diagnosis.
What else can mimic endometriosis?
A normal scan should not end the conversation. Persistent pelvic pain should not automatically be labelled endometriosis either. Overlaps include adenomyosis, fibroids, pelvic infection, ovarian cysts, irritable bowel syndrome, bladder pain syndrome, pelvic floor dysfunction, neuropathic pain, and other bowel or urinary conditions. A careful work-up sorts possibilities. It does not force every symptom into one name.
Pitfalls and limits to keep in mind
- Imaging does not see everything. Superficial peritoneal lesions are often invisible. A negative scan in a very symptomatic woman is not the same as “no endometriosis.”
- A normal examination does not close the case either.
- Delay remains real. Per De Corte et al., BJOG 2025, reported times range from a few months to more than 12 years across countries — even in well-organised systems.
- Operator experience matters. IDEA ultrasound and MRI quality depend heavily on who performs them.
- Adenomyosis commonly coexists with endometriosis and should be looked for deliberately because it may influence management.
In practice
- Start with history and examination. Then ask for a first-line IDEA-protocol transvaginal ultrasound with an experienced sonographer — or another imaging route if a vaginal scan is not appropriate.
- Add specialist pelvic MRI when ultrasound is inconclusive and symptoms remain suggestive, or when deep disease needs detailed mapping.
- Do not use CA-125 to screen, confirm, exclude or routinely monitor endometriosis.
- Discuss empirical hormonal treatment only when pain control is the priority and pregnancy is not being actively attempted.
- When pregnancy is the goal, prioritise fertility assessment — age, ovarian reserve, tubes, semen analysis, duration of infertility — over hormonal suppression.
- Reserve laparoscopy for situations where the findings would change care: a therapeutic need, unresolved symptoms after a proper assessment, or a carefully selected infertility scenario.
FAQ
Does endometriosis show up on ultrasound?
Often yes — especially ovarian endometriomas and many deep lesions — when a trained operator uses the IDEA protocol. Ultrasound may miss superficial peritoneal lesions. A normal scan does not close the case if symptoms remain strong.
Does a normal ultrasound rule out endometriosis?
No. Ultrasound may miss superficial disease and early lesions. If symptoms remain suggestive, specialist imaging, a fertility-focused work-up, or — when pregnancy is not the goal — an empirical pain-control trial may be discussed before writing the problem off.
Should ultrasound be performed during menstruation?
No. An IDEA-protocol ultrasound can generally be performed at any stage of the menstrual cycle. There is no strict cycle window required for a reliable examination, although timing may be adjusted for comfort, bleeding or local practice.
Why is my doctor not ordering CA-125?
Because it does not usefully screen, confirm, exclude or routinely monitor endometriosis. It is often normal early on, and it rises in many unrelated situations. ESHRE 2022 advises against biomarkers such as CA-125 in this diagnostic context.
Is MRI systematic after ultrasound?
No. If IDEA ultrasound is conclusive — a clear endometrioma, clear deep signs, or a reassuring scan that fits the clinical picture — MRI is not mandatory. It helps when ultrasound is inconclusive, when deep disease is suspected, or when a multidisciplinary plan needs more detail.
Will I need a laparoscopy to confirm the diagnosis?
Not routinely. Guidelines avoid automatic diagnostic laparoscopy. It may still be considered if imaging is negative despite strong ongoing suspicion, if empirical treatment has failed or is unsuitable, or if surgery is independently needed for pain, deep disease or a selected infertility scenario.
How long does diagnosis take?
With a coordinated pathway — a clinician familiar with endometriosis, an experienced sonographer, MRI when needed — a working diagnosis can emerge within weeks. Delay remains a global problem. If symptoms persist, it is reasonable to ask for a systematic evaluation rather than waiting indefinitely.
Sources
- Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open 2022;2022(2):hoac009.
- National Institute for Health and Care Excellence. Endometriosis: diagnosis and management (NG73). Updated 2024.
- Guerriero S, Condous G, van den Bosch T, et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis (IDEA consensus). Ultrasound Obstet Gynecol 2016;48:318–332.
- Kanti FS, Gorak Savard R, Bergeron F, et al. Transvaginal ultrasound and magnetic resonance imaging in the diagnosis of endometrioma: a systematic review and meta-analysis. J Obstet Gynaecol 2024;44(1):2311664.
- Xu Z, Li Y, Wang Y, Wan Y, Chen J. Transvaginal ultrasound and magnetic resonance imaging in detecting rectosigmoid deep infiltrating endometriosis: a comparative meta-analysis. Frontiers in Medicine 2025;12:1552185.
- Keckstein J, Saridogan E, Ulrich UA, et al. The #Enzian classification: A comprehensive non-invasive and surgical description system for endometriosis. Acta Obstet Gynecol Scand 2021;100:1165–1175.
- De Corte P, Klinghardt M, von Stockum S, Heinemann K. Time to Diagnose Endometriosis: Current Status, Challenges and Regional Characteristics — A Systematic Literature Review. BJOG 2025;132:118–130. doi:10.1111/1471-0528.17973.
Add as a Preferred Source on Google
You can add draksoyivf.com as one of your preferred health information sources on Google.

The content has been created by Dr. Senai Aksoy and medically approved.