Endometriosis: Symptoms, Diagnosis, Treatment and Fertility
Key Takeaways
Endometriosis is estimated to affect about 10% of women of reproductive age. A normal ultrasound does not exclude it. Not every endometrioma needs surgery, and endometriosis does not mean infertility. Hormonal treatments can reduce pain but do not treat infertility while you are trying to conceive. Under ESHRE 2022 and NICE 2024, diagnosis usually starts with imaging; routine endometrioma surgery before IVF has not been shown to improve live-birth rates.
Key evidence: ESHRE guideline: endometriosis (2022) WHO endometriosis fact sheet (2023) NICE NG73 — endometriosis (updated 2024)
Endometriosis: symptoms, diagnosis, treatment and fertility
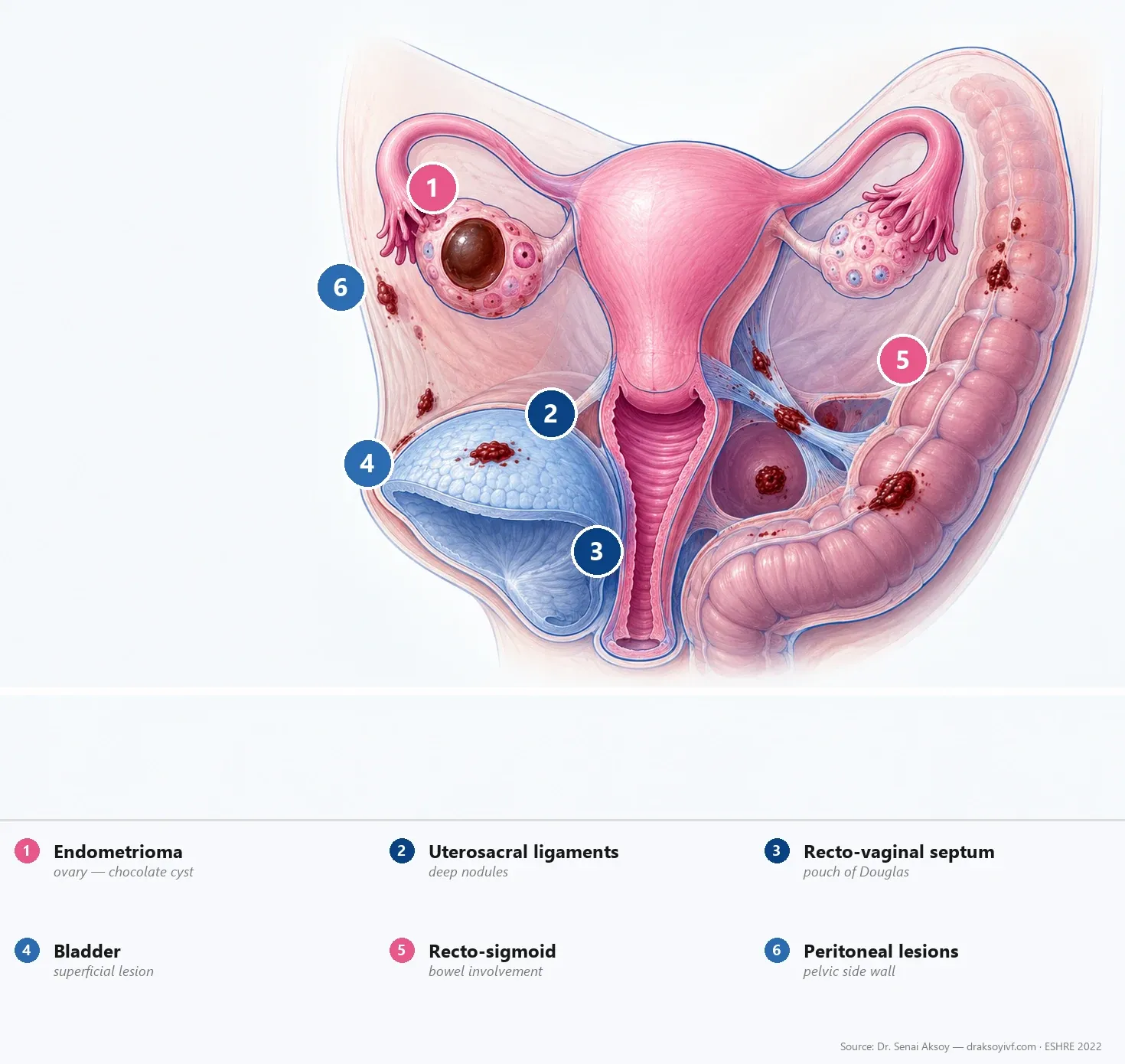
Endometriosis is a chronic inflammatory disease. Tissue similar to the lining of the uterus is found outside the womb — most often on the pelvic peritoneum, ovaries, ligaments, bowel or bladder, and sometimes farther away. It responds to estrogen and, over time, can leave scarring.
About 10% of women of reproductive age worldwide are thought to be affected — close to 190 million people, according to the WHO 2023 fact sheet. Published rates vary with how the diagnosis is made and who is studied. Work that only counts already-recorded diagnoses often reports lower figures.
This page is a full overview. For a narrower read: symptoms, diagnosis and ultrasound, pain treatment, endometriosis and infertility, endometrioma, and surgery. Related fertility reading: ovarian stimulation, egg freezing, IVF success overview, and adenomyosis and IVF.
What matters most at the start:
- A normal ultrasound does not exclude endometriosis.
- Not every endometrioma needs an operation.
- Endometriosis does not mean infertility.
- Hormonal treatments can ease pain, but they do not improve fertility while you are taking them.
- Routine endometrioma surgery before IVF has not been shown to improve live-birth rates.
Day-to-day care is shaped by two guidelines: ESHRE 2022 and NICE NG73 (updated 2024). Imaging usually comes first. Laparoscopy is no longer an automatic first diagnostic step. Long “ultralong” courses of GnRH agonist before IVF are not recommended as routine care (Cochrane 2019).
If your priority is pregnancy, you are not on the same path as someone whose priority is pain control. That difference should guide every next step.
Contents
- Numbers and delay
- Why it develops
- Classifications
- Symptoms
- Diagnosis
- Ovarian endometrioma
- Infertility and IVF
- Pain treatment
- Surgery
- Adolescents
- Turkish context
- Practical takeaways
- FAQ

Endometriosis in numbers
The familiar ~10% figure for women of reproductive age remains the best population estimate for patients (WHO 2023).
Other published rates look different because they measure different things. A systematic review by Parazzini et al., 2020 found pooled general-population estimates around 4.4%, about 23.8% in some surgical infertility series, and roughly half in some chronic-pelvic-pain surgical series — with wide confidence intervals. Those numbers describe selected study groups, not one “true” prevalence for every reader.
Genetics matter as well. Genetic studies estimate heritability at around 50% (Rahmioglu et al., 2023). That figure describes the genetic share of variation in a population. It does not mean a mother has a 50% chance of passing endometriosis to her daughter. The same work mapped 42 risk loci, with overlap into migraine, widespread pain, asthma and osteoarthritis.
Waiting for a diagnosis is still common. De Corte et al., BJOG 2025 reported delays from a few months to more than 12 years, depending on country and definition.
Pathophysiology: why endometriosis develops
No single theory explains every case — and that honesty matters when patients ask “why me?”
Retrograde menstruation (Sampson’s idea) is one plausible mechanism: period blood flows back through the tubes into the pelvis. The process is common, yet only some women develop endometriosis. It may contribute, but it has not been shown to be necessary in every case, and it does not explain the disease alone.
Other hypotheses include coelomic metaplasia (cells changing type), embryonic Müllerian remnants, stem-cell spread, immune dysregulation, genetic risk, and local changes in the endometrium such as progesterone resistance. Microbiome research is still early. Routine gut or vaginal microbiome testing, antibiotics or probiotics cannot currently be recommended as endometriosis treatment.
Adenomyosis can sit alongside endometriosis, but it is not the same disease. It involves the uterine muscle wall and can change treatment and fertility planning on its own — see adenomyosis and IVF.
Classifications: understanding the stages
Doctors use three complementary systems. None of them is a perfect map of how you feel day to day.
r-ASRM
This is the surgical score most people recognise. Stages I–II describe more limited superficial disease. Stages III–IV generally reflect more extensive disease, larger endometriomas and denser adhesions. Deep endometriosis may coexist at any stage and is not described well by the r-ASRM score. Stage often lines up poorly with pain or fertility.
#Enzian
#Enzian (2021) describes anatomical compartments. It can be applied to imaging as well as surgical findings, which makes it useful for mapping deep disease.
Endometriosis Fertility Index (EFI)
The EFI (Adamson & Pasta, 2010) combines history with surgical findings to discuss the chance of pregnancy without IVF after an operation. It is a conversation tool, not a stand-alone “wait / go to IVF” algorithm. Age, ovarian reserve, how long you have been trying, tubes, semen analysis, prior surgery and your priorities still decide timing.
Symptoms
Symptoms vary widely. Some women have none.
Common clues include period pain that worsens over time, pelvic pain outside the period, deep pain with intercourse, pain when opening the bowels or passing urine around the period, fatigue, bloating, cyclic rectal bleeding or blood in the urine, and difficulty conceiving.
Endometriosis can reduce fertility — but not every woman with endometriosis is infertile, and many conceive without assisted treatment.
On examination, tender ligaments, nodules behind the uterus, a fixed retroverted uterus or an ovarian mass can support suspicion. A normal examination still does not exclude endometriosis.
Diagnosis: imaging first
This is the practical shift in ESHRE 2022, echoed by NICE 2024: start with imaging, not with laparoscopy by default. More detail lives in our diagnosis guide.
A normal ultrasound does not exclude endometriosis.
Ultrasound is especially useful for ovarian endometriomas and many deep lesions. Superficial peritoneal endometriosis may be invisible. NICE still recommends offering ultrasound when endometriosis is suspected, even if the examination feels normal.
Transvaginal ultrasound (IDEA)
The IDEA protocol (Guerriero et al., 2016) gives the scan a structure: uterus and ovaries (including adenomyosis clues and endometriomas); soft markers; the sliding sign; then a search for deep nodules. Soft markers support suspicion; they are not specific. A free sliding sign does not rule out adhesions elsewhere.
Pelvic MRI
MRI helps when ultrasound is unclear, deep disease is suspected, or a surgical map is needed. It shares the same weakness for tiny superficial lesions.
CA-125
CA-125 is not for screening. It does not confirm or exclude endometriosis, and it is not for routine monitoring. It may appear in a broader work-up of an atypical ovarian mass — never alone.
Laparoscopy
Under ESHRE 2022, laparoscopy is no longer the default first diagnostic step. It remains useful when surgical treatment is indicated, or when symptoms persist despite normal imaging and empirical treatment is unsuccessful, unsuitable or declined (NICE 2024).
Ovarian endometrioma: operate or not?
An endometrioma — sometimes called a chocolate cyst — rarely has a one-size answer. Current guidance does not support a universal size cut-off for surgery (British Fertility Society ART recommendations, 2024).
Crossing a single centimetre mark is not, by itself, a reason to operate. The decision weighs pain, ultrasound appearance, growth, ovarian reserve, previous ovarian surgery, whether one or both ovaries are involved, and whether the cyst blocks safe access to follicles at egg retrieval.
Impact on ovarian reserve
Removing the cyst (cystectomy) can lower AMH. Meta-analyses consistently report an average fall in AMH after cystectomy, with a greater decline after bilateral or repeat surgery (Raffi et al., 2012; Somigliana et al., 2012). These group averages cannot predict the loss for an individual patient. Risk is also higher when surgery is poorly tissue-sparing.
Before IVF: routine surgery has not been shown to improve live birth
ESHRE’s strong recommendation is clear: do not perform routine endometrioma cystectomy before IVF simply to improve the live-birth rate. Hamdan et al., 2015 found no clear gain versus expectant care, while reserve may fall.
When I still discuss surgery before IVF
I discuss surgery mainly for uncontrolled pain, concern about malignancy, organ compromise such as ureteric obstruction or significant bowel stenosis, or anatomy that prevents safe egg retrieval. I do not recommend routine endometrioma surgery only to raise pregnancy rates.
My approach before IVF
I do not operate on an endometrioma simply because it is there, or because it has crossed a single size threshold. Before recommending surgery, I look at pain, ultrasound appearance, growth, previous ovarian surgery, AMH and antral follicle count, whether one or both ovaries are involved, and whether the cyst prevents safe access to follicles. If ovarian reserve is already limited, avoiding unnecessary surgery — and unnecessary delay — becomes especially important.
Surgical technique when an operation is needed
When surgery is necessary, the priority is complete and safe treatment while preserving healthy ovarian tissue. Excessive thermal coagulation should be avoided. Haemostasis should use the least ovarian damage that is reasonably possible. For ovarian endometriomas, cystectomy is generally more effective for pain and recurrence than drainage and coagulation alone — but the possible cost to reserve must stay in the conversation.
Endometriosis and infertility
Possible mechanisms include adhesions and tubal distortion, an altered inflammatory environment, reduced ovarian reserve and, in some studies, differences in oocyte or endometrial biology. Reserve may already be lower before any surgery (Muzii et al., 2018). How much individual molecular “receptivity” findings matter in clinic remains uncertain, and they do not justify routine receptivity testing.
Hormonal suppression can reduce pain, but it does not improve spontaneous pregnancy rates while you are trying to conceive.
Pain care and fertility care are different pathways (NICE).
Wait or move to IVF?
How long to wait after surgery is not decided by stage or EFI alone. Age, ovarian reserve, how long you have been trying, tubes, semen analysis, prior operations and your priorities are weighed together. EFI can support that talk; it does not replace it.
When reserve is already clearly reduced — especially if further ovarian surgery is planned — fertility planning should not be put off without reason. IVF or fertility-preservation options are individualised by age, expected egg yield and time pressure. Fixed laboratory cut-offs (for example one AMH or AFC number paired with DuoStim or embryo banking) are too blunt for a patient page.
Long GnRH-agonist pretreatment before IVF
This is not recommended as routine to improve IVF success. Cochrane 2019 found very-low-quality evidence and no clear live-birth benefit. It may still be used for pain control in selected patients. That is different from prescribing it routinely to improve IVF success.
Choice of IVF protocol
ESHRE does not mandate one ART protocol for endometriosis. Agonist and antagonist regimens can both be offered.
Freeze-all is not a routine endometriosis indication. Freezing embryos may make sense for cycle-specific reasons — OHSS risk, a premature progesterone rise, endometrial or medical issues, or planned genetic testing — not simply because disease is labelled “severe” or receptivity feels uncertain.
Fertility preservation
It is worth discussing when both ovaries are involved, only one ovary remains, ovarian surgery may be repeated, a young woman has extensive ovarian disease, or planned surgery clearly threatens reserve. Egg freezing is not mandatory for every endometrioma. Expected benefit depends on age and how many oocytes are likely to be collected — see how many eggs to freeze.
Pain management
Your doctor chooses according to pain intensity, pregnancy plans, other health issues and how well you tolerate treatment. Hormonal suppression treats pain, not infertility.
First-line options
Combined hormonal contraceptives and progestogens (including dienogest, a levonorgestrel IUD and other suitable progestogens) are both among the first-line choices in ESHRE 2022. Simple analgesics or NSAIDs can help on difficult days. Dienogest is a strong progestogen option (Strowitzki et al., 2010); it is not a compulsory “step two after the pill” for every woman.
If first-line care is not enough
GnRH agonists — or, where available and appropriate, oral GnRH antagonists — usually come next, with add-back to limit low-estrogen effects and bone loss. NICE technology appraisals have evaluated combinations such as relugolix–estradiol–norethisterone and linzagolix with add-back for selected adults after previous medical or surgical treatment. Access, cost, side effects and pregnancy plans matter.
Selected refractory cases
Aromatase inhibitors may be considered in selected resistant situations, usually together with another hormonal suppressant, and with clear counselling about off-label use in premenopausal women.
Supportive approaches
Pelvic-floor physiotherapy, psychological support, exercise or acupuncture may help some women manage symptoms — especially if examination shows myofascial pain or pelvic-floor dysfunction. ESHRE does not issue a specific recommendation that these approaches reduce endometriosis pain for all patients; the benefit–harm balance remains uncertain. They do not treat lesions and must not replace medical or surgical care when that care is needed.
Surgery: choosing the right technique
Excision or ablation for superficial disease
For pain reduction, excision may be considered when expertise allows. Evidence is limited and does not prove absolute superiority for every lesion (ESHRE 2022; Pundir et al., 2017; Healey et al., 2014). Technique should follow lesion site, depth, neighbouring organs and surgical experience. Excision can provide tissue for histology; ablation may be appropriate in some contexts.
Deep endometriosis
Deep disease involving bowel, bladder or ureters belongs in an experienced multidisciplinary centre with dedicated imaging.
Shaving or discoid excision can carry lower complication rates than segmental resection in suitably selected lesions (Bendifallah et al., 2020). Large, multifocal, stenosing or deeply transmural bowel disease may still need segmental resection. Complication rates alone cannot decide the best technique for every patient.
Recurrence
Without medical suppression after surgery, reported five-year recurrence rates vary widely — often approaching 40–50% in some series — depending on whether “recurrence” means symptoms, imaging findings or repeat surgery. Postoperative hormonal suppression reduces recurrence when pregnancy is not wanted straight away.
Endometriosis in adolescents
Endometriosis can begin with the first periods. Severe period pain, missed school or pain that does not respond to standard painkillers should raise the question early. Lesions may look red or vesicular rather than classically “pigmented.”
Early assessment and appropriate hormonal treatment can control pain and reduce disruption to school and daily life. Hormonal treatment has not been shown to preserve future fertility or to stop disease progression with certainty (ESHRE 2022). Surgery stays for refractory cases in expert hands. Fertility preservation may be discussed in selected severe ovarian disease, but who benefits — and by how much — remains uncertain.
Turkish context
Turkish law does not allow oocyte, sperm or embryo donation, or surrogacy. Because donation is not permitted in Turkey, treatment available locally must use the patient’s own oocytes. In very low-reserve situations, whether treatment remains medically reasonable still needs an individual assessment. Information about options abroad is informational only.
Practical takeaways
- Start with structured imaging; a normal scan does not exclude superficial disease.
- Do not use CA-125 to screen, confirm, exclude or routinely monitor.
- Do not operate every endometrioma — and not for a centimetre threshold alone.
- Before IVF, reserve surgery mainly for uncontrolled pain, concern about malignancy, organ compromise, or blocked follicular access.
- Hormones treat pain, not infertility while you are trying to conceive.
- First-line pain care includes combined contraceptives or progestogens; GnRH agents come later when needed.
- Surgical technique follows the lesion and the team — not a slogan.
- Deep disease or complex fertility plans need a joined-up team discussion.
There is no single pathway that fits every woman.
FAQ
Can endometriosis be cured?
There is no definitive cure, but symptoms can be controlled for long periods. Pregnancy is not a treatment method. Symptoms may ease in pregnancy or after menopause for some women, stay the same, or — less often — continue or worsen. Disease can remain active after menopause in some patients.
Can I have endometriosis even if my ultrasound and MRI are normal?
Yes. Expert ultrasound and MRI are useful for ovarian endometriomas and deep endometriosis, but superficial disease may remain invisible. Persistent symptoms should be assessed clinically rather than dismissed only because imaging looks normal.
Should every endometriosis be operated?
No. Pain, pregnancy plans, age and lesion location all matter. Routine surgery before IVF has been narrowed for good reason.
Why isn’t laparoscopy used for every diagnosis?
Skilled ultrasound and MRI map many endometriomas and deep lesions. They still miss much superficial disease. Laparoscopy stays for unresolved cases, or when treatment and diagnosis belong together.
Why not operate my endometrioma before IVF?
Because studies have not clearly shown that live-birth rates improve after routine pre-IVF cystectomy, and reserve can fall. Surgery remains an option for severe pain, suspected malignancy, organ compromise, or a cyst that blocks safe egg collection.
Which pain treatment fits which situation?
First-line options include combined hormonal contraceptives or progestogens, with painkillers as needed — when you are not trying to conceive. If those are not enough, GnRH agonists or, where available, oral GnRH antagonists with add-back may be discussed. Your doctor matches the choice to your symptoms, plans and tolerability.
How long after surgery before IVF?
Not by stage or EFI alone. Age, reserve, how long you have been trying, tubes, semen analysis and priorities decide together. EFI can help frame the conversation.
Can IVF make endometriosis worse?
Current data do not show that ovarian stimulation clearly increases endometriosis recurrence. The IVF decision is still individualised by age, reserve, pain and disease extent.
What if my reserve is already very low?
Do not put off the reproductive discussion, especially if further ovarian surgery is planned. Whether treatment remains medically reasonable — and which own-oocyte strategy fits — still needs an individual assessment. In Turkey, donation is not available.
What should I bring to the consultation?
Bring imaging reports (ultrasound, MRI), any previous fertility or hormone results — particularly AMH and antral follicle count reports when fertility is a concern — operative notes, current medicines, a pain and cycle diary, and a semen analysis if available.
Sources
- Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open 2022;2022(2):hoac009.
- National Institute for Health and Care Excellence. Endometriosis: diagnosis and management (NG73). Updated 2024.
- National Institute for Health and Care Excellence. Relugolix–estradiol–norethisterone for treating symptoms of endometriosis (TA1057). 2025.
- National Institute for Health and Care Excellence. Linzagolix for treating symptoms of endometriosis (TA1067). 2025.
- WHO. Endometriosis Fact Sheet, March 2023.
- Guerriero S, Condous G, van den Bosch T, et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis (IDEA consensus). Ultrasound Obstet Gynecol 2016;48:318–332.
- Parazzini F, Roncella E, Cipriani S, et al. The frequency of endometriosis in the general and selected populations: a systematic review. J Endometr Pelvic Pain Disord 2020;12(3–4):176–189.
- Rahmioglu N, Mortlock S, Ghiasi M, et al. The genetic basis of endometriosis and comorbidity with other pain and inflammatory conditions. Nat Genet 2023;55:423–436.
- Keckstein J, Saridogan E, Ulrich UA, et al. The #Enzian classification. Acta Obstet Gynecol Scand 2021;100:1165–1175.
- Adamson GD, Pasta DJ. Endometriosis fertility index. Fertil Steril 2010;94(5):1609–1615.
- De Corte P, Klinghardt M, von Stockum S, Heinemann K. Time to Diagnose Endometriosis. BJOG 2025;132:118–130. doi:10.1111/1471-0528.17973.
- Skorupskaite K, Hardy MF, Bhandari H, et al. Evidence based management of patients with endometriosis undergoing assisted conception: British Fertility Society policy and practice recommendations. Human Fertility 2024;27(1):2288634.
- Hamdan M, Dunselman G, Li TC, Cheong Y. The impact of endometrioma on IVF/ICSI outcomes. Hum Reprod Update 2015;21(6):809–825.
- Raffi F, Metwally M, Amer S. The impact of excision of ovarian endometrioma on ovarian reserve. J Clin Endocrinol Metab 2012;97(9):3146–3154.
- Somigliana E, Berlanda N, Benaglia L, et al. Surgical excision of endometriomas and ovarian reserve. Fertil Steril 2012;98(6):1531–1538.
- Muzii L, Di Tucci C, Di Feliciantonio M, et al. Antimüllerian hormone is reduced in the presence of ovarian endometriomas. Fertil Steril 2018;110(5):932–940.e1.
- Georgiou EX, Melo P, Baker PE, et al. Long-term GnRH agonist therapy before IVF for endometriosis. Cochrane Database Syst Rev 2019;CD013240.
- Pundir J, Omanwa K, Kovoor E, et al. Laparoscopic excision versus ablation for endometriosis-associated pain. J Minim Invasive Gynecol 2017;24(5):747–756.
- Healey M, Cheng C, Kaur H. To excise or ablate endometriosis?. J Minim Invasive Gynecol 2014;21(6):999–1004.
- Bendifallah S, Vesale E, Daraï E, et al. Bowel-sparing techniques versus segmental resection. J Minim Invasive Gynecol 2020.
- Strowitzki T, Marr J, Gerlinger C, et al. Dienogest versus leuprolide for endometriosis pain. Hum Reprod 2010;25(3):633–641.
- Sanchez AM, Vanni VS, Bartiromo L, et al. Is the oocyte quality affected by endometriosis?. Hum Reprod Update 2017;23(5):600–622.
Add as a Preferred Source on Google
You can add draksoyivf.com as one of your preferred health information sources on Google.

The content has been created by Dr. Senai Aksoy and medically approved.