Hyperprolactinemia: High Prolactin Levels in Women
Key Takeaways
A high prolactin result does not automatically mean that a prolactinoma is present. Testing is not routine for women with regular cycles and no suggestive symptoms. A moderate elevation should usually be repeated under suitable conditions and checked for macroprolactin. When treatment is needed, cabergoline is generally the first choice.
Key evidence: ESHRE unexplained infertility guideline (2023) Pituitary Society prolactinoma consensus (2023) Systematic review of macroprolactinaemia prevalence (2020)
On this page
- What a high result means
- Causes and testing
- Dr Aksoy’s perspective on borderline results
- The diagnostic workup
- Treatment options
- IVF and prolactin
- Pregnancy and prolactinoma
- Frequently asked questions
Receiving a high prolactin result can be unsettling, especially when it is only slightly above the laboratory range. The number alone does not establish a diagnosis. The first question is usually not “Which treatment do I need?”, but “Is this result reliable, and does it fit the symptoms?”
What high prolactin means in 2023 guidelines
Short answer: A high prolactin result must be interpreted alongside symptoms and the conditions in which the blood sample was taken. One result does not prove that a pituitary tumour is present.
When prolactin is high on a blood test, the medical name is hyperprolactinemia. The number alone is not a diagnosis of a pituitary tumour. Context, repeat testing, and symptoms decide what follows.
- Universal prolactin screening during every fertility assessment is not supported. The ESHRE 2023 Unexplained Infertility Guideline recommends against routine prolactin testing in women with regular cycles and unexplained infertility. Testing is targeted to menstrual irregularity, galactorrhea, anovulation, or signs of pituitary disease.
- Cabergoline is the first-line medical treatment endorsed by the 2023 Pituitary Society International Consensus and the 2011 Endocrine Society Clinical Practice Guideline.
- Macroprolactin — a biologically inactive form of prolactin — accounts for approximately 19% of hyperprolactinemic cases (international meta-analysis, 67 studies, 27 countries). Recognizing it prevents unnecessary medication and imaging.
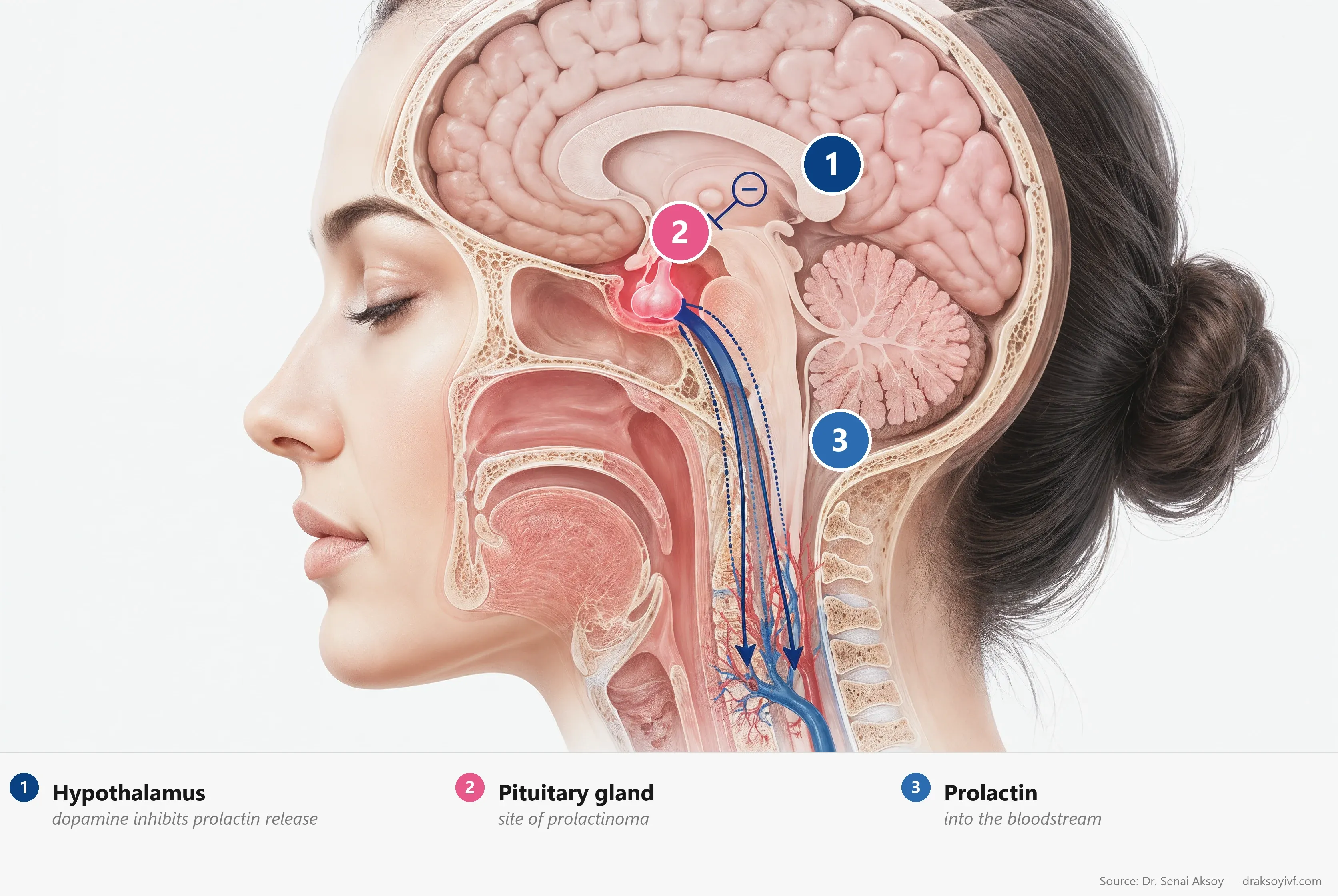

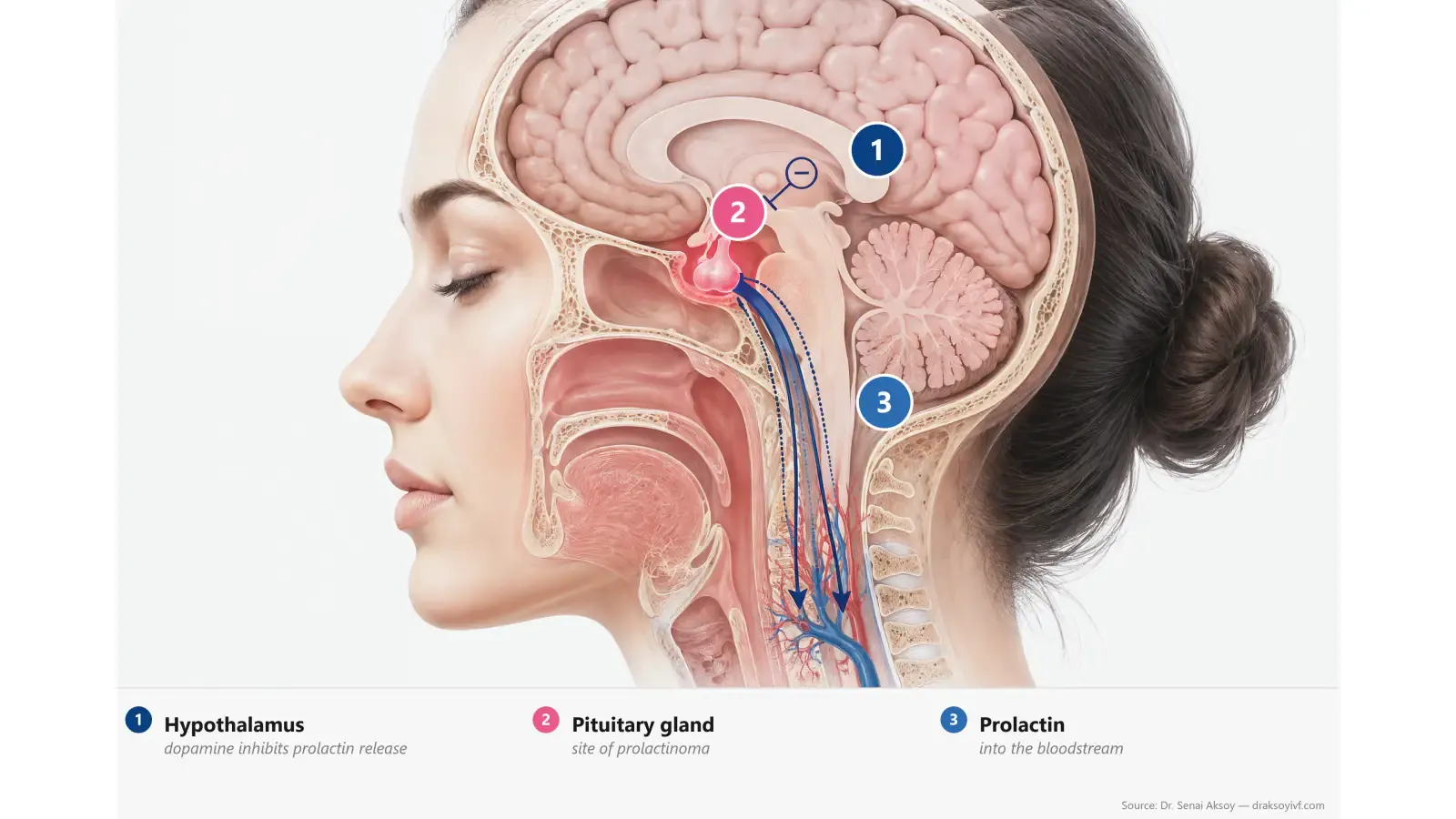
Prolactin: role and regulation
Short answer: Prolactin is best known for supporting milk production. Outside pregnancy and breastfeeding, its level is usually low.
Prolactin is a hormone produced by the anterior pituitary gland. Its main role is to prepare the breast and support milk production after childbirth. Its secretion is normally held in check by dopamine from the hypothalamus, so anything that blocks dopamine can raise prolactin levels.
Outside pregnancy and breastfeeding, prolactin stays low. Stress, sleep, nipple stimulation, intense exercise — and even the stress of a blood draw itself — can transiently raise it. The Pituitary Society 2023 Consensus notes that venipuncture stress alone can cause a two- to four-fold rise lasting under an hour. This is why a single prolactin result must always be interpreted in context.
Hyperprolactinemia vs prolactinoma: not the same thing
Short answer: Hyperprolactinemia is a laboratory finding. A prolactinoma is only one of several possible causes.
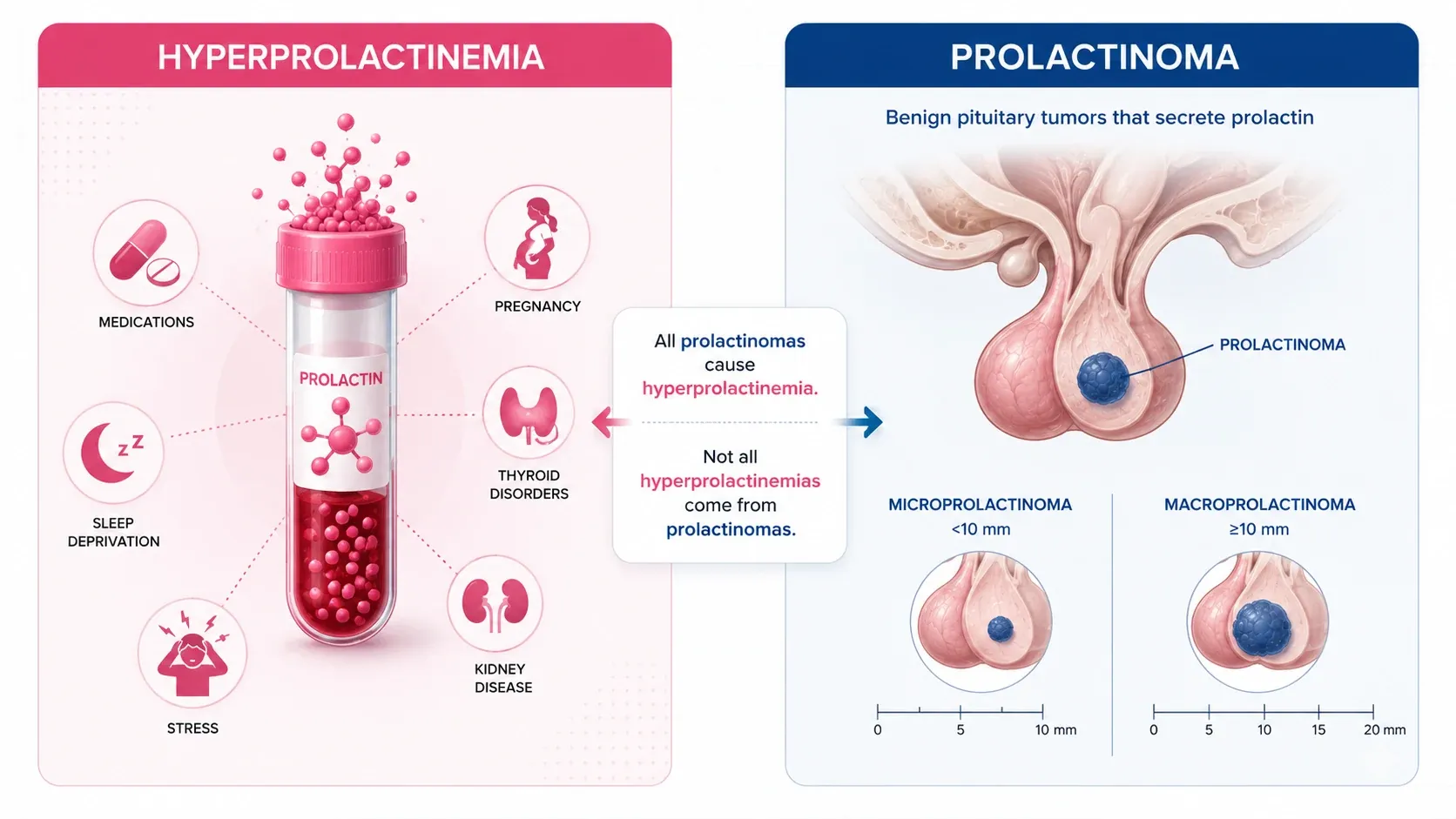
Hyperprolactinemia is a biological finding: a prolactin level above the normal range. It has many possible causes, some of them entirely physiological.
A prolactinoma is one specific cause: a benign pituitary adenoma that secretes prolactin. They are classified by size:
- Microprolactinoma (under 10 mm),
- Macroprolactinoma (10 mm or larger), which can compress neighboring structures.
As a clinical rule of thumb, the Pituitary Society 2023 notes that a prolactin level above 200 ng/mL strongly suggests a prolactinoma. Levels below 200 ng/mL require active consideration of other causes — medications, hypothyroidism, or macroprolactin. This distinction guides the decision to order an MRI.
Causes of hyperprolactinemia
Short answer: Before discussing treatment, it is important to understand why prolactin is high. The cause may be physiological, medication-related, hormonal, or pituitary.
Identifying the cause precedes any treatment.
Physiological causes
Pregnancy, breastfeeding, nipple stimulation, sleep, stress, recent intercourse, intense exercise, high-protein meals, alcohol — any of these can transiently raise prolactin. A modestly elevated value often justifies a repeat measurement under better conditions before further workup.
Medication-related causes
Many medications elevate prolactin, mostly by blocking dopamine’s inhibitory effect:
- Antipsychotics — risperidone and paliperidone are the most prolactin-raising; haloperidol, amisulpride, olanzapine carry moderate risk; aripiprazole, quetiapine and clozapine have less effect.
- Antiemetics and prokinetics: metoclopramide, domperidone.
- Antidepressants: SSRIs (modest effect), tricyclics, MAOIs.
- Other: opioids, verapamil, methyldopa, high-dose estrogens, high-dose H2 antihistamines.
A suspected medication should never be stopped on your own. Only the team that prescribed it can weigh the benefit-risk balance and propose an alternative.
Medical causes
- Prolactinoma and other pituitary adenomas (stalk effect: prolactin usually below 100 ng/mL when the tumor doesn’t secrete prolactin itself).
- Primary hypothyroidism — through indirect stimulation via TRH.
- Chronic kidney disease (reduced clearance).
- Cirrhosis.
- Chest-wall lesions: shingles, post-thoracotomy, severe burns.
- Idiopathic hyperprolactinemia: about 40% of cases, many of which turn out to be macroprolactin.
Macroprolactin: the diagnostic pitfall to know
Macroprolactin is a complex between prolactin and an immunoglobulin (IgG). Standard prolactin assays detect it, but it has little biological activity and rarely explains symptoms on its own.
Its frequency is underestimated: a meta-analysis of 67 studies across 27 countries (Che Soh et al., 2020) found a pooled prevalence of 18.9% (95% CI 15.8–22.1) in hyperprolactinemic patients. In infertile women specifically, prevalence reaches 11–13%.
The Pituitary Society 2023 strongly recommends (translated quote): “Macroprolactinemia should be evaluated in patients with moderately increased serum levels of prolactin (<200 ng/mL), at least in those with discordant clinical or imaging findings.” The standard method is PEG precipitation at the laboratory: less than 40% monomer recovery defines macroprolactinemia. Thinking of it before starting treatment avoids unnecessary medication and pituitary MRI.
Clinical Note
When should prolactin actually be tested?
Short answer: Prolactin is not measured routinely in every fertility assessment. Testing becomes useful when cycle changes, symptoms, or the clinical context suggest a prolactin disorder.
This is the most important shift in the 2023 guidelines. Prolactin testing is not routine in the infertility workup.
The ESHRE 2023 Unexplained Infertility Guideline (Romualdi et al., Hum Reprod) explicitly recommends against routine prolactin testing in women with regular cycles and unexplained infertility. A recent UK fertility-clinic cohort (Zargar-Shoshtari et al., 2022) showed that mostly mild hyperprolactinemia had no impact on ongoing pregnancy or live-birth rates (OR 0.8; 95% CI 0.5–1.1). This held true in both ovulatory and oligo-anovulatory subfertile women.
Dr Aksoy’s clinical perspective
“The cases that require the most judgement are often not the very high results, but the borderline ones — roughly 50% above the laboratory’s upper limit. Scientific societies rightly advise against measuring prolactin without a clinical indication. Yet many women arrive with a result already in hand, and the number itself creates uncertainty.
“In women with polycystic ovary syndrome (PCOS), mild elevations have historically been attributed in part to the oestrogenic environment. I prefer to interpret these results in a wider clinical frame, because routine laboratory reference intervals are not specific to women with PCOS. That does not mean automatically treating a raised value as normal. A 2025 cross-sectional study found that hyperprolactinaemia was no more common in women with PCOS than in controls; most mild elevations were explained by venepuncture stress or macroprolactin. In practice, I first confirm the measurement under suitable conditions, then review symptoms, medicines, thyroid function and macroprolactin before labelling disease or starting treatment.”
Prolactin testing is justified in these situations:
- irregular cycles, oligomenorrhea or amenorrhea,
- galactorrhea (milky discharge outside breastfeeding),
- documented anovulation,
- headaches or visual changes suggesting a pituitary adenoma,
- polycystic ovary syndrome workup (prolactin is part of the differential per the 2023 International PCOS Guideline),
- women on antipsychotics or other prolactin-raising medications with hormonal symptoms.
For recurrent pregnancy loss, the 2026 ASRM Practice Committee opinion concludes that high-quality evidence linking prolactin disturbances to recurrent miscarriage is lacking. It does not recommend routine testing unless symptoms such as galactorrhea or anovulation are also present.
Symptoms of high prolactin in women
Short answer: The first signs are often irregular cycles, absent ovulation, or unexpected milk discharge rather than one dramatic symptom.
In women
Symptoms of high prolactin levels in females often start with cycle changes rather than a dramatic single complaint:
- Irregular or absent cycles (oligomenorrhea, amenorrhea).
- Anovulation and difficulty conceiving.
- Galactorrhea: spontaneous or expressed milky discharge outside breastfeeding.
- Decreased libido (sex drive), vaginal dryness, mood changes.
In men
- Decreased libido, erectile dysfunction.
- Possible changes in semen parameters (concentration, motility, morphology).
- Rarely, gynecomastia.
Symptoms related to a pituitary tumor
When a macroprolactinoma compresses neighboring structures, persistent headaches and visual disturbances (visual-field narrowing from optic chiasm compression) can appear. Other pituitary hormone deficiencies may coexist and should be investigated.
Longer-term consequences
Sustained hyperprolactinemia can lead to estrogen or testosterone deficiency, with potential impact on bone health (demineralization), mood, sleep, and sexual function. These dimensions deserve to be named in follow-up.
Mechanism: why prolactin blocks ovulation
Short answer: Persistently high prolactin can interrupt the hormonal conversation between the brain and the ovaries, making ovulation less regular or stopping it altogether.
The mechanism is now well established: elevated prolactin inhibits kisspeptin neurons in the arcuate nucleus of the hypothalamus. These neurons — now recognized as the master regulators of reproduction — project onto GnRH neurons and govern GnRH pulse frequency.
A landmark study (Brown et al., Endocrinology 2019) showed that selectively deleting the prolactin receptor on arcuate kisspeptin neurons abolishes prolactin’s suppression of LH pulses. In women with hyperprolactinemia, administering kisspeptin can restore LH pulsatility (Hoskova et al., JCEM 2022).
The cascade is: kisspeptin → GnRH → FSH/LH → estradiol → ovulation. Any disruption of GnRH pulsatility impairs follicular development and ovulation. Normalizing prolactin restores ovulation in more than 80% of women with overt hyperprolactinemic amenorrhea.
Diagnosis: the practical workup
Short answer: The result is confirmed first. Simple explanations are then checked before a pituitary MRI is considered. This sequence helps avoid medicalising a temporary rise.
1. Confirm the measurement
The Pituitary Society 2023 recommends (translated quote): “Patients with hyperprolactinemia but serum levels of prolactin less than five times the upper limit of normal should undergo repeat prolactin testing. Cannulated prolactin sampling is recommended if an influence of stress is suspected.”
In practice:
- follow the laboratory’s instructions and sit quietly before a mid-morning sample,
- no intense exercise, no nipple stimulation, no heavy meal in the preceding 1–2 hours,
- repeat any modestly elevated value under rested conditions before further workup; if stress remains a concern, a sample taken through an indwelling cannula can help.
2. Rule out the obvious
- TSH to rule out hypothyroidism.
- Urea/creatinine and liver function tests as appropriate.
- β-hCG to rule out pregnancy.
- Full medication review.
- Test for macroprolactin (PEG precipitation) if prolactin is moderately elevated (below 200 ng/mL) or if symptoms and imaging are discordant.
3. Pituitary MRI
The Pituitary Society 2023 strongly recommends a dynamic gadolinium-enhanced pituitary MRI (macrocyclic chelates preferred) in patients with confirmed hyperprolactinemia that cannot be explained by a non-adenomatous cause, to monitor response to medical therapy, and to establish baseline status 3–6 months after surgery.
4. The hook effect: a pitfall to know
For very large adenomas, some assays can underestimate prolactin because of an assay saturation effect known as the “hook effect.” This affects approximately 5% of macroprolactinomas and up to 14% of giant adenomas. The Pituitary Society 2023 strongly recommends (translated quote): “In patients with giant adenoma and typical features of hyperprolactinemia but normal or slightly elevated serum levels of prolactin, samples should be re-measured after 1:100 dilution to exclude a high-dose hook effect.”
5. Visual field testing
Indicated when imaging shows the adenoma touches or compresses the optic chiasm. During pregnancy, visual fields are checked each trimester for macroadenomas; only on symptoms for microadenomas.
Treatment: cabergoline first-line
Short answer: When medication is indicated, cabergoline is generally the preferred first treatment. The cause, symptoms, and any pituitary finding still guide the plan.
Cabergoline
Cabergoline is the dopamine agonist recommended as first-line therapy by the Pituitary Society 2023 and the Endocrine Society. It mimics dopamine’s inhibitory action on prolactin.
- The dose is determined and adjusted by your doctor based on prolactin level, the presence and size of any prolactinoma, and individual tolerance. Treatment usually begins at a low dose, taken once or twice a week, and is gradually titrated.
- Tolerability is usually good; the most common side effects (nausea, headache, postural dizziness) are most often transient.
- Ovulation often returns once prolactin is normalised. Pregnancy chances then depend on age and other fertility factors as well as prolactin.
The pivotal trial (Webster et al., NEJM 1994) showed that cabergoline normalized prolactin in 83% of patients vs 59% on bromocriptine, and restored ovulation and pregnancy in 72% vs 52%.
Bromocriptine
Bromocriptine, usually taken in the evening and titrated by the prescribing physician, remains an option — particularly when already well tolerated, or in certain pregnancy contexts, given its very large historical safety database (over 6,000 documented pregnancies). Its tolerability is markedly worse than cabergoline: in the 1994 NEJM trial, 78% of bromocriptine patients reported adverse events and 12% stopped treatment due to intolerance.
Quinagolide
Quinagolide is a non-ergot alternative useful in patients intolerant to cabergoline. It is not available in all countries.
Treating the underlying cause
- Hypothyroidism: thyroid hormone replacement can normalize prolactin on its own.
- Causative medication: the prescribing team evaluates adjustment or substitution, never abrupt discontinuation without specialist input.
- Chronic kidney disease or other chronic illness: management of the primary disease shapes the trajectory.
Cardiac surveillance: should you be concerned?
Ergot-derived dopamine agonists have been associated with cardiac valvulopathy when used at high doses, notably in Parkinson’s disease. At the doses used in hyperprolactinemia, which are much lower, the available data are reassuring:
- a meta-analysis (Stiles et al., JCEM 2018) found an increased prevalence of subclinical tricuspid regurgitation (OR 3.74; 95% CI 1.79–7.8), without clinically significant valvulopathy;
- a large primary-care cohort study (Stiles et al., JCEM 2021) found no excess heart failure or valve repair.
The Pituitary Society 2023 considers routine echocardiographic screening unnecessary at endocrine doses. A baseline echocardiogram may be offered by your doctor before long-term therapy, without systematic repeat screening at usual doses.
Surgery and radiotherapy
Transsphenoidal surgery is reserved for selected situations:
- resistance or intolerance to dopamine agonists,
- cystic adenomas (often poor response to medical therapy),
- persistent optic chiasm compression,
- cerebrospinal fluid leak,
- macroprolactinoma in a woman planning multiple pregnancies: the Pituitary Society 2023 notes that pre-conceptional debulking surgery reduces the risk of symptomatic tumor enlargement in pregnancy from 21% to 4.7%.
A systematic review of 25 surgical studies (Zamanipoor Najafabadi et al., JCEM 2020) reported long-term remission in 67% of prolactinoma surgeries overall and 83% for microprolactinomas.
Radiotherapy is much rarer, reserved for aggressive or persistent tumors that fail other approaches.
Resistance to medical therapy
Dopamine agonist resistance is defined as failure to normalize prolactin or to achieve ≥50% tumor shrinkage at the maximum tolerated dose. Prevalence is approximately 10% for cabergoline and 20–30% for bromocriptine (Maiter, Neuroendocrinology 2019). Management options include dose escalation, switching to cabergoline (from bromocriptine), surgery, and more rarely radiotherapy or temozolomide for aggressive cases.
Hyperprolactinemia and IVF
Short answer: A mild, symptom-free elevation does not automatically need treatment before IVF. A confirmed prolactin disorder that affects ovulation or reflects a prolactinoma is a different situation.
Should mild hyperprolactinemia be treated before IVF?
No high-quality evidence supports routine treatment of mild asymptomatic hyperprolactinemia before IVF. Multiple retrospective IVF series show that mild basal prolactin elevations do not impair fertilization, implantation, or live birth.
Transient elevations during ovarian stimulation
Prolactin rises driven by increasing estradiol during ovarian stimulation are physiological. The Sonigo et al. 2023 review found no adverse effect on oocyte number, fertilisation, or pregnancy. There is no indication to start a dopamine agonist for a temporary, stimulation-related rise.
Continuing treatment during stimulation
For a patient already on treatment, cabergoline is generally continued at the lowest effective dose through stimulation and oocyte retrieval, then adjusted at confirmation of pregnancy depending on adenoma status.
Cabergoline for OHSS prevention
This is a distinct but related indication. A Cochrane review found that a short course of cabergoline, started around the hCG trigger according to the IVF team’s protocol, reduced moderate-to-severe OHSS (RR 0.38; 95% CI 0.29–0.51) without reducing clinical pregnancy.
Hyperprolactinemia, prolactinoma and pregnancy
Short answer: Most microprolactinomas remain stable during pregnancy. Larger or invasive adenomas need an individual monitoring and treatment plan.
Tumor-growth risk during pregnancy
Pregnancy estrogens can stimulate prolactinoma growth. The risk depends on tumor type:
- Microprolactinoma: about 3% symptomatic growth.
- Untreated macroprolactinoma: 21–32%.
- Macroprolactinoma after surgery or radiotherapy: about 4.8%.
Pituitary Society 2023 recommendations
- Microprolactinoma and non-invasive intrasellar macroprolactinoma: dopamine agonist is stopped at confirmation of pregnancy.
- Invasive macroprolactinoma or chiasmal proximity: continuing treatment through pregnancy may be considered; pre-conceptional debulking surgery is an alternative.
- Visual field testing: each trimester for macroadenomas, only on symptoms for microadenomas.
- MRI without gadolinium: performed if new headaches or visual changes develop.
- Prolactin measurement is not informative during pregnancy (physiological elevation).
- Reintroduction of dopamine agonist to be considered for clinically significant adenoma growth.
Cabergoline safety in early pregnancy
More than 1,300 cabergoline-exposed pregnancies have been described in historical series, including Lebbe et al. (2010). The 2025 Chakraborty meta-analysis of 1,387 pregnancies (PMID 40629810) and the 2025 Otis systematic review (PMID 40116053) found no increase in major malformations with first-trimester exposure. This safety signal does not mean treatment should automatically continue after pregnancy is confirmed; the decision depends on adenoma size and clinical risk.
Bromocriptine retains the largest historical pregnancy database (more than 6,000 documented pregnancies) — an acceptable alternative, particularly when already well tolerated before pregnancy.
Breastfeeding
Breastfeeding is not contraindicated for a stable microprolactinoma or non-progressive macroprolactinoma. Dopamine agonists suppress lactation and are usually withheld during breastfeeding, except in case of tumor growth.
Before conception
The Endocrine Society 2011 and Pituitary Society 2023 recommendations converge: achieve stable normoprolactinemia and two to three regular menstrual cycles before active attempts at conception. This allows accurate dating of any subsequent pregnancy and planning of treatment management.
Quality of life and support
Short answer: The impact is not limited to a laboratory value. Symptoms can affect sexual health, confidence, relationships, and the emotional experience of fertility treatment.
Hyperprolactinemia can affect a couple’s relationship, sexual health, and fertility journey. Erectile difficulties in men, cycle disturbances and galactorrhea in women, mood changes, and fatigue all deserve attention. Psychological support can be useful, especially when symptoms become part of a longer fertility or IVF journey.
In practice
Short answer: A high prolactin result is a signal to understand, not a diagnosis by itself. The most useful next step is often confirmation rather than immediate treatment.
Hyperprolactinemia is not a disease in itself — it is a sign that should prompt the search for a cause. The key shifts in the 2023 guidelines are:
- do not test prolactin routinely in every fertility assessment — test when symptoms or clinical signs suggest it,
- always think of macroprolactin when prolactin is moderately elevated and symptoms are absent or discordant,
- cabergoline as first-line when medical treatment is indicated,
- stop treatment at confirmation of pregnancy for microadenomas and most non-invasive macroadenomas, with appropriate surveillance,
- do not treat stimulation-related transient prolactin rises or mild asymptomatic hyperprolactinemia before IVF.
Most hyperprolactinemias respond well once the cause is identified. Fertility can be restored when prolactin is normalized, though there is no automatic guarantee if other infertility factors coexist.
FAQ
Should prolactin be tested in every fertility assessment?
No. ESHRE 2023 recommends against routine prolactin testing in women with regular cycles and unexplained infertility. Testing is indicated in case of cycle disturbances, galactorrhea, anovulation, pituitary symptoms, or polycystic ovary syndrome.
Is a moderately elevated prolactin always pathological?
Not necessarily. Stress, the blood draw itself, short sleep, a protein-rich meal, certain medications, or macroprolactin can all explain a moderate elevation. A repeat measurement under better conditions, sometimes with macroprolactin testing, is often the first step.
What is macroprolactin and why does it matter?
Macroprolactin is a complex between prolactin and an immunoglobulin. It is detected by standard assays but has no significant biological effect. It accounts for about 19% of hyperprolactinemic cases. PEG precipitation testing prevents unnecessary medication and pituitary MRI.
When is a pituitary MRI ordered?
When prolactin is confirmed elevated without an obvious non-adenomatous cause, for headaches or visual changes, for prolonged amenorrhea, or to monitor response to treatment. For very large tumors with paradoxically low prolactin, a 1:100 dilution of the assay is requested to rule out a “hook effect.”
Cabergoline or bromocriptine: which to choose?
Cabergoline is first-line per the Pituitary Society 2023 and Endocrine Society 2011: it normalizes prolactin in 83% of patients (vs 59% for bromocriptine) with better tolerability. Bromocriptine retains specific indications, particularly when already well tolerated or because of its larger historical pregnancy safety database.
Can you get pregnant on cabergoline?
Yes — that is often the goal. Once prolactin is normalized and ovulation returns, conception becomes possible. At confirmation of pregnancy, cabergoline is usually stopped for microadenomas and non-invasive intrasellar macroadenomas. Accumulated data on more than 1,300 cabergoline-exposed pregnancies show no increase in major malformations.
Should mild hyperprolactinemia be treated before IVF?
Without symptoms (cycle disturbances, galactorrhea) and with moderate elevation, there is no evidence that treatment improves IVF outcomes. Stimulation-related transient prolactin rises are physiological and do not justify starting a dopamine agonist.
Sources
- Petersenn S, Fleseriu M, Casanueva FF, et al. Diagnosis and management of prolactin-secreting pituitary adenomas: a Pituitary Society international Consensus Statement. Nat Rev Endocrinol 2023;19(12):722–740.
- Melmed S, Casanueva FF, Hoffman AR, et al. Diagnosis and Treatment of Hyperprolactinemia: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2011;96(2):273–288.
- Romualdi D, Ata B, Bhattacharya S, et al. (ESHRE Guideline Group). Evidence-based guideline: unexplained infertility. Hum Reprod 2023;38(10):1881–1890.
- Teede HJ, Tay CT, Laven JSE, et al. Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. J Clin Endocrinol Metab 2023;108(10):2447–2469.
- Luque-Ramírez M, Quintero-Tobar A, Martínez-García MÁ, et al. Mild hyperprolactinemia in women with polycystic ovary syndrome: insights from a large cross-sectional study. J Clin Transl Endocrinol 2025;41:100412.
- Che Soh NAA, Yaacob NM, Omar J, et al. Global prevalence of macroprolactinemia among patients with hyperprolactinemia: a systematic review and meta-analysis. Int J Environ Res Public Health 2020;17(21):8199.
- Webster J, Piscitelli G, Polli A, et al. A comparison of cabergoline and bromocriptine in the treatment of hyperprolactinemic amenorrhea. N Engl J Med 1994;331:904–909.
- Stiles CE, Tetteh-Wayoe ET, Bestwick JP, et al. Meta-analysis of the prevalence of cardiac valvulopathy in patients with hyperprolactinemia treated with cabergoline. J Clin Endocrinol Metab 2018;104(2):523–538.
- Brown RSE, Herbison AE, Grattan DR. Acute suppression of LH secretion by prolactin in female mice is mediated by kisspeptin neurons in the arcuate nucleus. Endocrinology 2019;160:1323–1332.
- Hoskova K, Bryant NK, Chen ME, et al. Kisspeptin overcomes GnRH neuronal suppression secondary to hyperprolactinemia in humans. J Clin Endocrinol Metab 2022;107(8):e3515–e3525.
- Stiles CE, Lloyd G, Bhattacharyya S, et al. Incidence of cabergoline-associated valvulopathy in primary care patients with prolactinoma using hard cardiac endpoints. J Clin Endocrinol Metab 2021;106(2):e711–e720.
- Zamanipoor Najafabadi AH, Zandbergen IM, de Vries F, et al. Surgery as a viable alternative first-line treatment for prolactinoma patients: a systematic review and meta-analysis. J Clin Endocrinol Metab 2020;105(3):e32–e41.
- American Society for Reproductive Medicine Practice Committee. Recurrent pregnancy loss: a committee opinion. Fertil Steril 2026.
- Tang H, Hunter T, Hu Y, et al. Cabergoline for preventing ovarian hyperstimulation syndrome. Cochrane Database Syst Rev 2012;(2):CD008605.
- Lebbe M, Hubinont C, Bernard P, Maiter D. Outcome of 100 pregnancies initiated under treatment with cabergoline in hyperprolactinaemic women. Clin Endocrinol 2010;73(2):236–242.
- Otis AS, et al. Cabergoline use and pregnancy outcomes: a systematic review. Birth Defects Res 2025;117(3):e2464.
- Chakraborty et al. Safety of cabergoline for prolactinoma in pregnancy: a systematic review and meta-analysis. Clin Endocrinol 2025.
- Zargar-Shoshtari S et al. Hyperprolactinemia and live-birth rates in a UK fertility-clinic cohort. Hum Fertil 2022;25:790.
- Maiter D. Management of Dopamine Agonist-Resistant Prolactinoma. Neuroendocrinology 2019;109(1):42–50.
- Sonigo C et al. Hyperprolactinemia and ART. Pharmaceuticals 2023;16:122.
Add as a Preferred Source on Google
You can add draksoyivf.com as one of your preferred health information sources on Google.

The content has been created by Dr. Senai Aksoy and medically approved.