Ovarian endometrioma: surveillance or surgery, and impact on fertility
Key Takeaways
An endometrioma (ovarian endometriosis cyst, sometimes called a 'chocolate cyst') has a characteristic 'ground-glass' ultrasound appearance. The choice between surveillance and surgery depends on size, clinical impact, fertility plans and any signs of atypia. Cystectomy reduces ovarian reserve by about 30 % after a unilateral procedure and 44 % after a bilateral procedure. Before IVF, routine surgery is not recommended because it does not improve live birth rates. Fertility preservation should be discussed early before any surgery in a young woman.
What is an endometrioma?
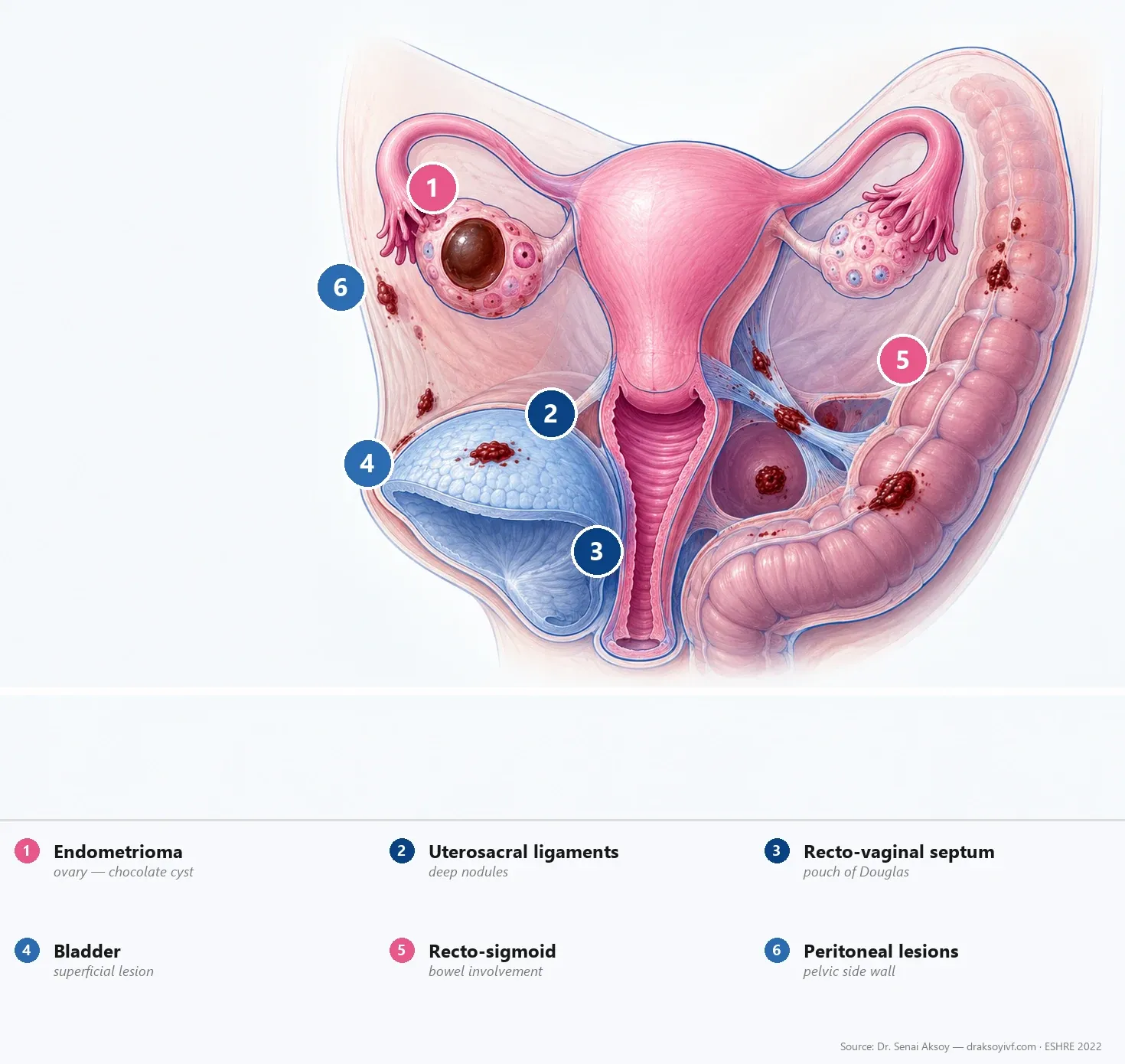
An endometrioma is an ovarian cyst formed by endometrial-like tissue that develops within the ovarian parenchyma. Its content is degraded old blood, which gives it the characteristic “chocolate cyst” appearance at surgery and a typical “ground-glass” ultrasound look (homogeneous, finely granular echogenicity, without septations or papillary projections).
It is a common manifestation of endometriosis, found in about 17 to 44 % of patients across series. Its presence usually implies more extensive disease in the pelvis — superficial peritoneal and deep endometriosis are frequently associated.
This article expands the endometrioma management section. For the overview, see the complete endometriosis guide; for fertility impact, see endometriosis and infertility; for surgical techniques, see endometriosis surgery.
Ultrasound features
A typical endometrioma shows several features on transvaginal ultrasound:
- Unilocular cyst (occasionally bi- or multilocular in older lesions);
- Homogeneous “ground-glass” content — finely echogenic, with no clear fluid plane;
- Regular wall, sometimes thickened;
- No intracystic papillary projection or atypically vascularised area on Doppler;
- Often associated with ovarian fixation or a negative sliding sign in the Pouch of Douglas.
The differential diagnosis includes the functional haemorrhagic cyst (which resolves in 6 to 8 weeks), dermoid cyst and, more rarely, ovarian cancer (raised by papillary projections, thick septations or atypical vascularity).
Surveillance or surgery?
The decision balances the expected benefit of surgery (pain relief, follicle access, ruling out malignancy) against the biological cost (lower ovarian reserve, surgical risks).
Indications for surveillance
- Asymptomatic unilateral endometrioma under 4 cm in a woman with fertility plans;
- Typical ultrasound features with no signs of atypia;
- Preserved ovarian reserve that should be protected;
- Patient accepting regular imaging follow-up.
Surveillance is done by transvaginal ultrasound every 6 to 12 months depending on context, with reassessment of symptoms and ovarian reserve (AMH, antral follicle count).
Indications for surgery
- Pain refractory to well-conducted medical treatment;
- Suspicion of malignancy: papillary projections, thick septations, atypical vascularity, rapid growth, aberrant markers;
- Cyst over 4 cm obstructing follicle access at IVF retrieval;
- Infection or haemoperitoneum;
- Documented progressive growth under surveillance.
The 4 cm threshold is not absolute: it is a practical landmark that must be balanced against fertility plans, ovarian reserve and symptoms.
Warning signs of malignancy
The risk of ovarian cancer (in particular clear-cell and endometrioid carcinomas) is slightly increased in women with endometriosis but remains low in absolute terms. Ultrasound signs suggestive of atypia include:
- intracystic papillary projections;
- thick or vascularised septations;
- solid component in a previously purely cystic lesion;
- atypical vascularity on Doppler;
- rapid growth documented on two close-interval scans;
- markedly raised CA-125 in this specific context (not for routine screening).
Any atypia warrants a pelvic MRI and an oncology consultation before any surgical decision.
Impact of cystectomy on ovarian reserve
Laparoscopic cystectomy of an endometrioma reduces ovarian reserve — a key point for decision making.
- Meta-analysis by Raffi et al., 2012: weighted mean drop in AMH of −1.13 ng/mL (95 % CI −1.88 to −0.37), with −30 % after unilateral cystectomy and −44 % after bilateral.
- Somigliana et al., 2012: 9 of 11 studies confirm this drop.
- Risk of premature ovarian insufficiency of 2.4 to 13 % after bilateral cystectomy.
Two mechanisms explain this:
- inadvertent removal of healthy ovarian tissue adherent to the cyst wall;
- thermal damage from bipolar coagulation used for haemostasis.
Note: the meta-analysis by Muzii et al., 2018 shows that the endometrioma itself is associated with lower AMH, independent of any surgery. Part of the “loss” of AMH attributed to cystectomy probably also reflects the biological effect of the cyst on the carrier ovary.
Before IVF: no routine surgery
This is the key change in the ESHRE 2022 recommendations. The Hamdan et al., 2015 meta-analysis found no benefit:
- Clinical pregnancy: OR 0.97 (95 % CI 0.78–1.20);
- Live birth: OR 0.90 (95 % CI 0.63–1.28);
- Response to stimulation: lower after surgery.
ESHRE 2022 issues a strong recommendation: routine cystectomy of endometriomas before IVF is not recommended.
Surgery remains discussed case-by-case to relieve pain, rule out suspected malignancy, or facilitate follicle access in case of a large cyst obstructing retrieval.
Fertility preservation before surgery
When surgery is judged necessary in a young woman without an ongoing pregnancy plan, fertility preservation should be discussed early:
- oocyte vitrification after ovarian stimulation;
- embryo vitrification if there is a parental plan with a stable partner;
- timing: ideally before surgery, particularly in bilateral endometrioma or after prior contralateral cystectomy.
The discussion also addresses the target oocyte count (often 15 to 20 mature oocytes for a reasonable chance of live birth) and the cost and availability of the technique in your setting.
Surgical techniques: sparing reserve
When surgery is indicated, several precautions limit ovarian reserve loss:
- Laparoscopic cystectomy rather than laparotomy;
- Minimal use of bipolar coagulation — prefer suture or haemostatic agents;
- Energy-sparing techniques: plasma energy or CO₂ laser for cyst-wall ablation when available;
- Careful identification of the cleavage plane to avoid tearing healthy ovarian tissue;
- Surgeon trained in endometriosis surgery.
See endometriosis surgery for technique details.
Recurrence after surgery
Endometrioma recurrence after cystectomy is estimated at about 21.5 % at 2 years and 30 to 50 % at 5 years without post-operative medical therapy. Risk factors include young age, high r-ASRM score, associated deep endometriosis and absence of pregnancy after surgery.
A maintenance hormonal treatment (continuous combined contraceptive, dienogest, LNG-IUS) significantly reduces recurrence and is offered after surgery in women without an immediate pregnancy plan.
Bilateral endometrioma: major caution
Bilateral endometrioma is a particularly delicate situation:
- bilateral cystectomy carries a non-negligible risk of premature ovarian insufficiency;
- fertility preservation should be systematically discussed before any procedure;
- a two-stage surgery (one side, then the other, with hormonal recovery in between) may be considered in selected situations;
- an experienced team is essential.
In practice
- A typical transvaginal ultrasound is usually enough; MRI complements in case of atypia or associated deep endometriosis.
- Surveillance is reasonable for an asymptomatic unilateral endometrioma under 4 cm without atypia in a woman with fertility plans.
- Surgery is indicated for refractory pain, suspected malignancy, a large cyst obstructing retrieval, or complications.
- No routine cystectomy before IVF; individualised decision.
- Fertility preservation to be discussed before any surgery in a young woman.
- Post-operative medical maintenance to reduce recurrence.
FAQ
Should every endometrioma be operated?
No. An asymptomatic unilateral endometrioma under 4 cm with typical ultrasound features in a woman with fertility plans can be monitored. Surgery is indicated for refractory pain, suspected malignancy, a large cyst obstructing follicle access, or complications.
Will my AMH drop after surgery?
Likely yes. Cystectomy reduces AMH by about 30 % after unilateral and 44 % after bilateral procedures on average. Part of this drop also reflects the biological effect of the cyst itself on the carrier ovary.
Should I have my endometrioma removed before IVF?
Not automatically. Studies do not show improved live birth after pre-IVF cystectomy. The discussion centres on pain, follicle access at retrieval and any suspicion of malignancy.
For how long should I monitor an endometrioma?
As long as the surveillance criteria hold (stable size under 4 cm, no atypia, no disabling pain, preserved ovarian reserve). Generally, ultrasounds every 6 to 12 months are enough, adjusted to clinical course and fertility plans.
Can my endometrioma become cancer?
The risk of ovarian cancer is slightly increased in women with endometriosis (especially clear-cell and endometrioid carcinomas) but remains low in absolute terms. Ultrasound signs of atypia (papillary projections, thick septations, solid component, atypical vascularity) should always raise the diagnosis and warrant a complementary MRI.
Should I freeze my eggs before surgery?
To be discussed with your team based on your age, current reserve, uni- or bilateral nature, and fertility plans. Preservation is particularly relevant before a bilateral cystectomy or in a young woman without an ongoing pregnancy plan.
What helps limit recurrence after surgery?
A maintenance hormonal therapy — continuous combined contraceptive, dienogest, or the levonorgestrel-releasing IUS — significantly reduces endometrioma recurrence and is offered after surgery in women without immediate pregnancy plans.
Sources
- Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open 2022;2022(2):hoac009.
- Hamdan M, Dunselman G, Li TC, Cheong Y. The impact of endometrioma on IVF/ICSI outcomes: a systematic review and meta-analysis. Hum Reprod Update 2015;21(6):809–825.
- Raffi F, Metwally M, Amer S. The impact of excision of ovarian endometrioma on ovarian reserve: a systematic review and meta-analysis. J Clin Endocrinol Metab 2012;97(9):3146–3154.
- Somigliana E, Berlanda N, Benaglia L, et al. Surgical excision of endometriomas and ovarian reserve: a systematic review on serum antimüllerian hormone level modifications. Fertil Steril 2012;98(6):1531–1538.
- Muzii L, Di Tucci C, Di Feliciantonio M, et al. Antimullerian hormone is reduced in the presence of ovarian endometriomas: a systematic review and meta-analysis. Fertil Steril 2018.
Add as a Preferred Source on Google
You can add draksoyivf.com as one of your preferred health information sources on Google.

The content has been created by Dr. Senai Aksoy and medically approved.