Endometriosis surgery: excision, deep disease and ovary-sparing techniques
Key Takeaways
For superficial endometriosis lesions, excision is preferred over thermal ablation (Pundir 2017, Healey 2014). Deep infiltrating endometriosis (rectum, sigmoid, ureters, bladder) should be managed in expert centres with multidisciplinary teams; bowel-sparing techniques (shaving, discoid excision) have markedly fewer complications than segmental resection (Bendifallah 2020). Recurrence is estimated at 21.5 % at 2 years and 40–50 % at 5 years without post-operative medical therapy and is significantly reduced by maintenance hormonal treatment.
Why operate — and why not routinely
Surgery is no longer mandatory in endometriosis. The ESHRE 2022 guideline (Becker et al., Human Reproduction Open) narrowed routine indications in favour of a medical and imaging-led approach. Surgery remains, however, an essential tool in several situations:
- pain refractory to well-conducted medical treatment;
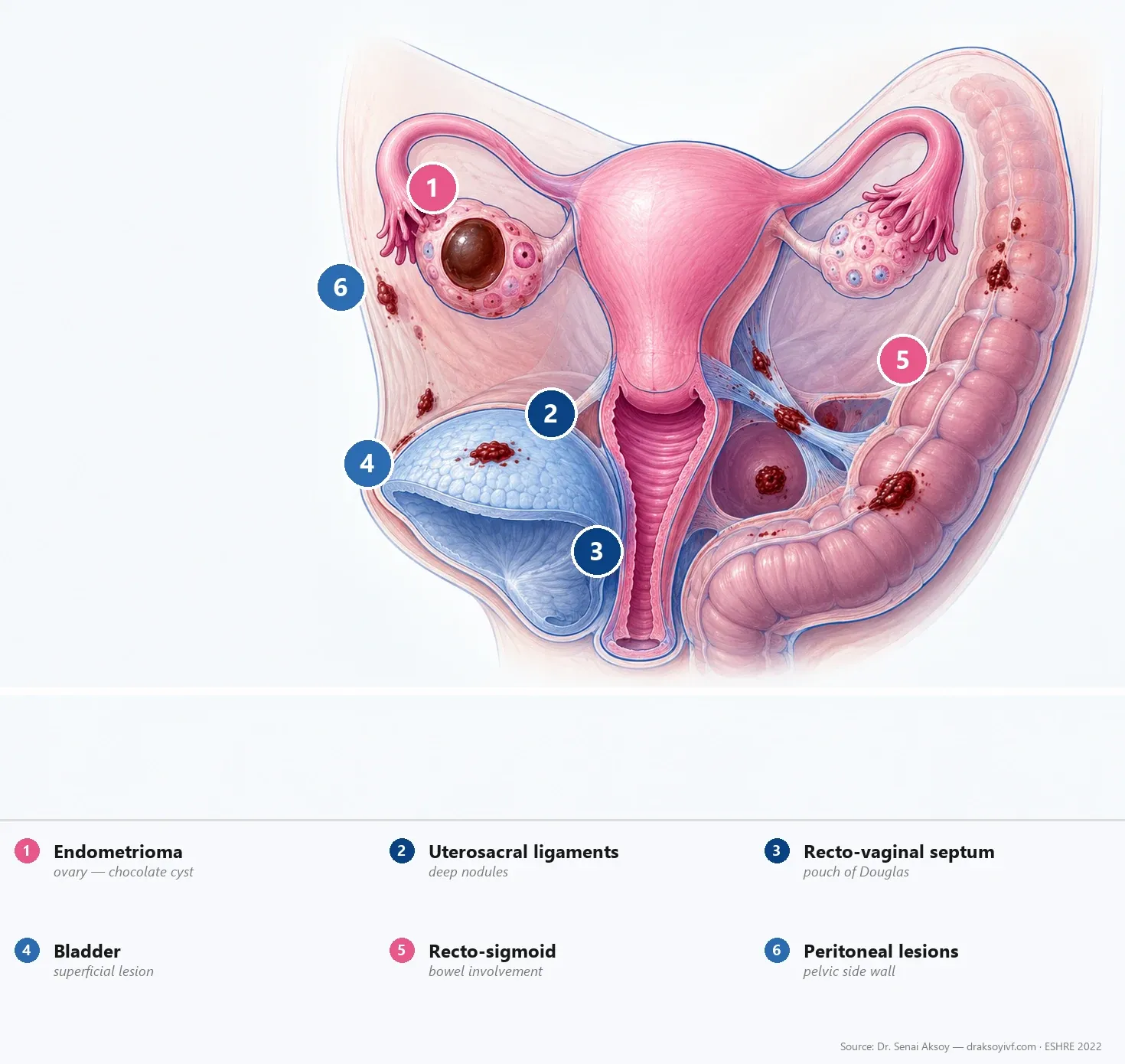
- deep infiltrating endometriosis (DIE) of the rectum, sigmoid, ureters, bladder, recto-vaginal septum;
- endometrioma that is symptomatic, large, or with signs of malignancy;
- associated infertility in selected situations;
- severe adhesions distorting pelvic anatomy.
Conversely, surgery should no longer be:
- a mandatory diagnostic step when imaging is conclusive;
- a reflex response before a properly conducted medical trial;
- a routine cystectomy of an endometrioma before IVF (see endometriosis and infertility).
This article details current techniques. For the overview, see the complete endometriosis guide.
Superficial lesions: excision over ablation
For superficial peritoneal lesions, two approaches are possible: excision (complete removal of the lesion with its peritoneal support) or ablation (thermal destruction by monopolar, bipolar, plasma or laser energy).
Excision is now preferred where expertise allows.
The evidence
- Pundir et al., 2017 meta-analysis: 3 randomised trials, 335 patients — excision superior at 12 months for dyschezia, chronic pelvic pain and the EHP-30 global score.
- Healey et al., 2014: 5-year randomised follow-up — excision superior for dyspareunia and lower need for long-term hormonal treatment.
The biological rationale
Excision offers several biological advantages over ablation:
- complete histology — diagnostic confirmation and possible search for atypia;
- less thermal injury to adjacent healthy tissue, particularly the ovary;
- less microscopic residue beneath the treated area.
The limitation remains operator expertise: excision is technically more demanding and must be performed by a trained surgeon.
Deep endometriosis: multidisciplinary team
Deep infiltrating endometriosis (DIE) is defined as lesions infiltrating the muscular layer of an organ (rectum, sigmoid, bladder, ureter, vagina, recto-vaginal septum) by more than 5 mm.
Its management should be centralised in expert centres with:
- dedicated pre-operative imaging (IDEA ultrasound + pelvic MRI) for mapping;
- a multidisciplinary team: gynaecological surgery, colorectal surgery, urological surgery, specialised anaesthesia;
- a standardised classification such as the #Enzian system (Keckstein et al., 2021) to describe involvement by compartment.
The pre-operative workup systematically includes a digestive assessment (recto-sigmoidoscopy or colo-MRI), a urological assessment (uro-MRI, ureteroscopy as indicated), and a functional workup as appropriate.
Bowel-sparing techniques
For rectal and sigmoid involvement, three techniques coexist:
Shaving
Superficial excision of the lesion without opening the bowel lumen. The most conservative technique.
Discoid excision
Excision of a disc comprising the full thickness of the bowel wall, followed by transverse suture. Moderately invasive.
Segmental resection
Resection of a bowel segment with end-to-end anastomosis. The most invasive — reserved for extensive, circumferential or multifocal involvement.
Comparative evidence
The Bendifallah et al., 2020 meta-analysis (60 studies) shows that shaving has significantly fewer complications than the more invasive techniques:
- Recto-vaginal fistula: OR 0.19 (95 % CI 0.10–0.36) vs disc; OR 0.26 (95 % CI 0.15–0.44) vs segmental resection.
- Anastomotic leak: OR 0.22 (95 % CI 0.06–0.73) vs disc.
- Persistent bladder dysfunction: OR 0.34 (95 % CI 0.18–0.63) vs segmental.
Analgesic efficacy of the three techniques is broadly comparable. Shaving is therefore preferred where anatomy allows, and segmental resection is reserved for extensive involvement without a conservative alternative.
Urinary tract involvement
Bladder
Bladder involvement is usually managed by a discoid excision of the bladder wall followed by a two-layer suture, with bladder catheterisation for 7 to 14 days depending on extent. The risk of vesico-vaginal fistula is low with careful technique.
Ureters
Ureteral involvement may be extrinsic (compression by peri-ureteral tissue) or intrinsic (infiltration of the wall). Procedures range from simple ureterolysis to resection-anastomosis or bladder reimplantation. Pre-operative ureteral stenting is common to secure the procedure.
Diaphragmatic and thoracic endometriosis
Diaphragmatic and pleural involvement is rare but possible — manifested by cyclic scapular pain or catamenial pneumothorax. Management often involves a thoracic surgery team in addition to the gynaecological team.
Choice of surgical energy
Several energy sources are used in endometriosis surgery:
- Monopolar: broadly used, good haemostasis but notable thermal diffusion.
- Bipolar: better precision, preferred over sensitive ovarian areas.
- Plasma energy: very limited thermal diffusion, useful for endometrioma cystectomy.
- CO₂ laser: sub-millimetric precision, little thermal diffusion, useful for superficial peritoneal lesions and cyst-wall ablation.
- Ultrasonic devices: used in colorectal surgery.
The choice depends on surgeon experience, operative site and equipment availability.
Surgical risks to keep in mind
Like any complex pelvic surgery, endometriosis surgery carries risks that should be clearly explained:
- Recurrence (see dedicated section);
- Ovarian insufficiency after cystectomy, especially bilateral (2.4–13 %);
- Recto-vaginal or vesico-vaginal fistula;
- Ureteral injury;
- Anastomotic leak after segmental resection;
- Persistent bladder dysfunction (urinary retention) after extensive pelvic surgery;
- Post-operative adhesions;
- standard anaesthetic complications.
The expertise level of the centre is one of the main modifiers of these risks.
Recurrence and prevention
Recurrence is estimated at about 21.5 % at 2 years and 40 to 50 % at 5 years without post-operative medical therapy. The rate depends on initial stage, completeness of excision, age and hormonal context.
Maintenance medical treatment significantly reduces recurrence risk:
- Continuous combined hormonal contraceptive;
- Dienogest 2 mg/day;
- Levonorgestrel-releasing IUS (LNG-IUS);
- or another progestin option as appropriate.
This treatment is offered after surgery in women without immediate pregnancy plans. See treating endometriosis pain.
Surgery and fertility
The effect of surgery on fertility depends on context:
- Stage I/II with superficial endometriosis: excision may modestly improve chances of spontaneous pregnancy.
- Stage III/IV with EFI ≥ 7: unassisted live-birth rate of about 60 % at 3 years after surgery.
- Endometrioma: routine cystectomy before IVF is not recommended because it does not improve live birth rate (see endometriosis and infertility).
- Severely diminished ovarian reserve: avoid ovarian surgery if possible, prioritise fertility preservation.
In practice
- Excision rather than ablation for superficial lesions where expertise allows.
- Deep endometriosis in expert centres with multidisciplinary teams and dedicated pre-operative imaging.
- Bowel-sparing techniques (shaving, discoid excision) preferred over segmental resection where anatomy allows.
- Endometrioma cystectomy not routine before IVF — individualised decision.
- Fertility preservation to be discussed before any ovarian surgery in a young woman.
- Post-operative hormonal maintenance to reduce recurrence.
FAQ
Why prefer excision over ablation?
Randomised studies (Pundir 2017, Healey 2014) show excision is superior for dyschezia, dyspareunia, chronic pelvic pain and overall quality-of-life scores. Excision also allows complete histology and limits thermal injury to healthy tissue.
Will I lose part of my bowel during surgery?
Not systematically. Conservative techniques (shaving, discoid excision) are preferred where anatomy allows. Segmental resection is reserved for extensive, circumferential or multifocal involvement. The Bendifallah 2020 meta-analysis shows that shaving has markedly fewer complications.
How long is the recovery after surgery?
For standard laparoscopic surgery of superficial endometriosis, return to normal activities takes 2 to 4 weeks. For DIE surgery with bowel or urological resection, recovery may take 6 to 8 weeks depending on extent.
What is the risk of recurrence after surgery?
About 21.5 % at 2 years and 40 to 50 % at 5 years without post-operative medical therapy. Risk is significantly reduced by maintenance hormonal therapy (continuous combined contraceptive, dienogest or LNG-IUS) in women without immediate pregnancy plans.
Should surgery be performed to improve fertility?
It depends on stage and context. Excision of superficial lesions may modestly improve chances of spontaneous pregnancy. Routine cystectomy of an endometrioma before IVF is not recommended. The decision is individualised by EFI, age, ovarian reserve and associated factors.
How do I choose where to have surgery?
For deep endometriosis, prefer an expert centre with:
- a multidisciplinary team (gynaecology, colorectal surgery, urology);
- sufficient surgical volume (several dozen cases per year);
- dedicated pre-operative imaging (IDEA ultrasound + MRI);
- an outcomes-assessment process.
Is there an alternative to surgery?
Yes. Stepped medical treatment (combined contraceptives, dienogest, GnRH agonists with add-back) is effective for most pain and should be tried before considering purely diagnostic surgery. Surgery remains indicated for refractory pain, symptomatic deep endometriosis, or complications.
Sources
- Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open 2022;2022(2):hoac009.
- Pundir J, Omanwa K, Kovoor E, et al. Laparoscopic Excision Versus Ablation for Endometriosis-associated Pain: An Updated Systematic Review and Meta-analysis. J Minim Invasive Gynecol 2017;24(5):747–756.
- Healey M, Cheng C, Kaur H. To excise or ablate endometriosis? A prospective randomized double-blinded trial after 5-year follow-up. J Minim Invasive Gynecol 2014;21(6):999–1004.
- Bendifallah S, Vesale E, Daraï E, et al. Bowel-sparing techniques versus segmental resection for deep infiltrating colorectal endometriosis: systematic review and meta-analysis. J Minim Invasive Gynecol 2020.
- Keckstein J, Saridogan E, Ulrich UA, et al. The #Enzian classification: A comprehensive non-invasive and surgical description system for endometriosis. Acta Obstet Gynecol Scand 2021;100:1165–1175.

The content has been created by Dr. Senai Aksoy and medically approved.