Endometriosis symptoms: recognising the signs and when to seek care
Key Takeaways
Endometriosis symptoms vary widely, are often cycle-dependent, and may combine progressive dysmenorrhoea, chronic pelvic pain, deep dyspareunia, dyschezia, dysuria and infertility.
Key evidence: ESHRE Guideline: Endometriosis (2022) Diagnostic Delay in Endometriosis: Systematic Review
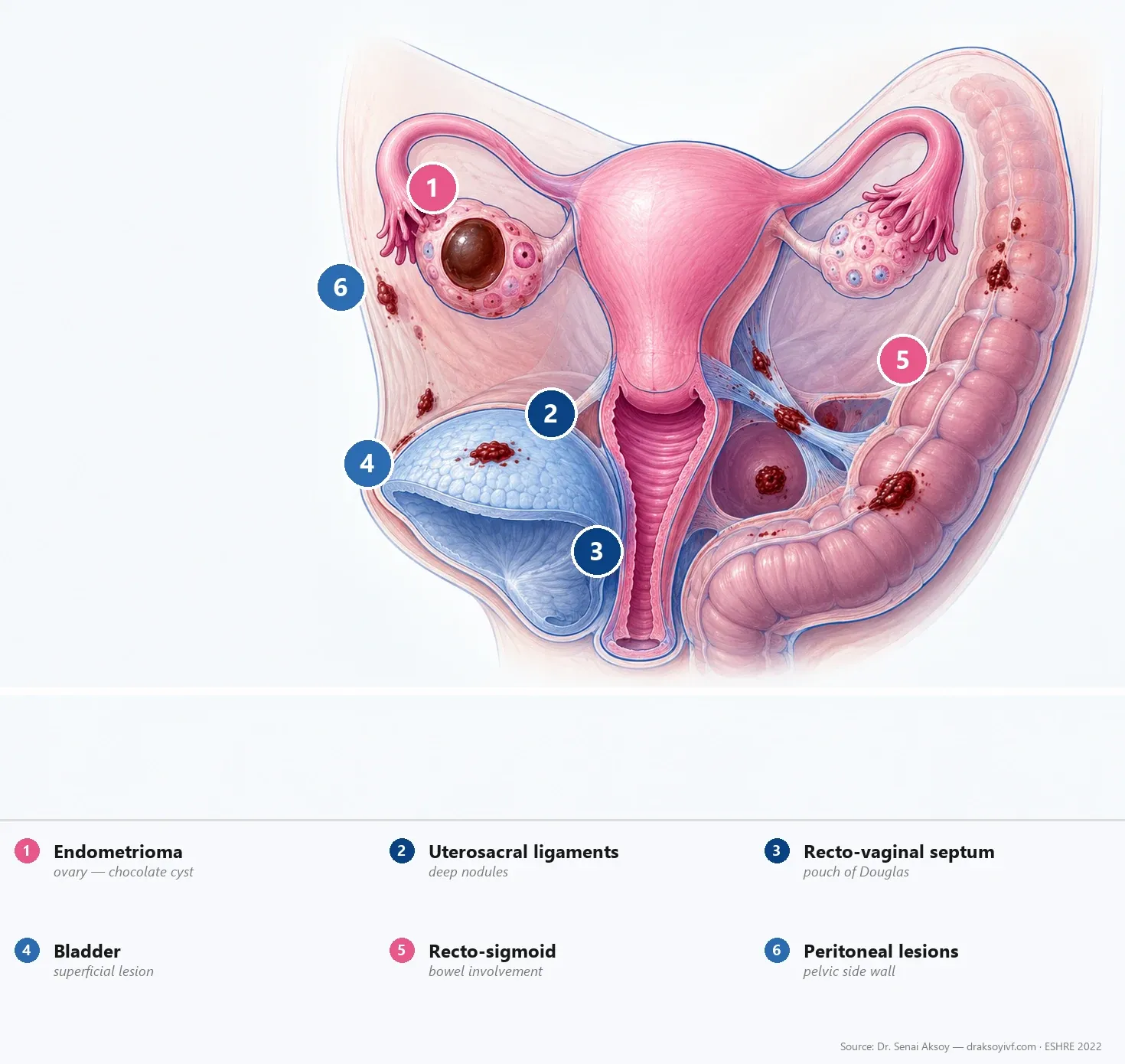
A highly variable presentation
Endometriosis symptoms vary significantly between individuals. Some patients experience severe pelvic pain despite small superficial implants, while others have large endometriomas discovered incidentally during routine fertility scans.
Symptom severity does not always correlate with lesion extent. Identifying key symptoms helps shorten the global diagnostic delay.
For detailed diagnostic evaluation, visit diagnosing endometriosis and our complete endometriosis guide.
Cardinal symptoms
Progressive Dysmenorrhea
- Worsening period pain: Painful periods that progressively intensify over time.
- Painkiller resistance: Severe menstrual cramps unresponsive to over-the-counter NSAIDs.
- Contrast with primary dysmenorrhea: Unlike common teenage period cramps, secondary dysmenorrhea caused by endometriosis escalates across menstrual cycles.
Chronic Pelvic Pain
- Constant or intermittent pelvic aching occurring outside of menstruation.
- May reflect localized nerve involvement or central pain sensitization over time.
Deep Dyspareunia
- Pain felt deep in the pelvis during or after sexual intercourse.
- Frequently indicates deep infiltrating nodules along the uterosacral ligaments or rectovaginal septum.
Dyschezia & Gastrointestinal Symptoms
- Painful bowel movements or rectal pressure during menstruation.
- Often accompanied by cyclic abdominal bloating, diarrhea, or constipation.
Dysuria
- Pain, pressure, or burning during urination during menstrual cycles.
- Suggests bladder wall implants or vesicouterine involvement.
Subfertility & Infertility
- Present in 30% to 50% of women diagnosed with endometriosis.
- Unexplained difficulty conceiving is often the initial trigger for diagnostic imaging.
Chronic Fatigue
- Persistent, debilitating exhaustion driven by chronic pelvic inflammation.
Atypical presentations to keep in mind
- Extra-pelvic sites: Cyclic shoulder or chest pain (diaphragmatic implants) or catamenial pneumothorax.
- Asymptomatic disease: Unexpected discovery during laparoscopic tubal testing or routine ultrasound.
- Overlapping conditions: Symptoms frequently mimic irritable bowel syndrome (IBS) or interstitial cystitis.
Clinical examination
Physical examination by a gynecologist may reveal:
- Tenderness along the uterosacral ligaments.
- Palpable nodules in the rectovaginal space.
- A fixed, retroverted uterus due to pelvic adhesions.
- Ovarian masses consistent with endometriomas.
A normal pelvic examination does not exclude early or superficial disease.
The adolescent: a particular case
Severe period pain causing school absence or emergency visits in teenagers warrants prompt medical evaluation.
- Initiate continuous oral contraceptives or progestins as first-line symptom control.
- Avoid unnecessary diagnostic surgery in young patients unless medical therapy fails.
The diagnostic delay: a global problem
Systematic reviews (De Corte et al. 2025) document average diagnostic delays of 6 to 11 years worldwide.
Contributing factors:
- Normalization of severe menstrual pain by society and healthcare providers.
- Multiple consultations across non-specialist disciplines (gastroenterology, urology).
- Non-specialist pelvic ultrasounds missing deep infiltrating implants.
ESHRE 2022 guidelines prioritize early IDEA-protocol ultrasound scanning to eliminate unnecessary delays.
Warning signs that warrant consultation
Seek medical evaluation if you experience:
- Period pain that progressively worsens or resists analgesics.
- Deep pelvic pain during intercourse.
- Painful defecation or urination synchronized with your menstrual cycle.
- Infertility after 12 months of trying (6 months if over age 35).
- Severe, disabling dysmenorrhea in adolescent family members.
In practice
- Recognize progressive dysmenorrhea and deep pelvic pain as primary indicators.
- Understand that normal scans or physical exams do not rule out superficial disease.
- Initiate early medical management for adolescent period pain.
- Request specialist IDEA-protocol ultrasound if symptoms persist.
FAQ
Are all painful periods suggestive of endometriosis?
No. Primary dysmenorrhoea — common in adolescents, stable over time and well controlled by NSAIDs — is not synonymous with endometriosis. The warning sign is dysmenorrhoea that worsens over the years, resists analgesics, or is accompanied by other features (dyspareunia, dyschezia, dysuria, infertility).
Can you have endometriosis without pain?
Yes. Some patients are diagnosed during an infertility workup, on imaging for another reason, or at surgery for another indication. Symptom severity does not always reflect disease extent.
Is my pain “in my head”?
No. Endometriosis pain is organic, linked to a chronically inflamed tissue producing its own pain mediators and sensitising the central nervous system over time. A psychological component to chronic pain exists, but it comes on top — not instead.
My 16-year-old daughter has very painful periods. When should we consult?
If the pain keeps her out of school, if she regularly takes painkillers, if pain lasts several days per cycle, or if she has had emergency-department visits for menstrual pain, consult without delay. ESHRE 2022 recommends first-line hormonal treatment in this context without necessarily waiting for surgical confirmation.
Which clinician should I see first?
A gynaecologist trained in endometriosis is ideal. Otherwise, your primary-care doctor can start the workup (transvaginal ultrasound under the IDEA protocol) and organise referral. Avoid fragmented care pathways (gastroenterologist + urologist + psychiatrist in parallel without coordination), which often delay diagnosis.
What should I bring to the consultation?
Bring your pelvic ultrasound and MRI reports, hormonal tests (AMH, FSH, oestradiol, prolactin), any operative reports, current medications, a pain diary over several cycles, and your partner’s semen analysis if infertility is part of the picture.
Sources
- Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open 2022;2022(2):hoac009.
- Diagnostic Delay in Endometriosis: Systematic Review
- WHO. Endometriosis Fact Sheet, March 2023.
- De Corte P, Klepsch S, Christ B, et al. Diagnostic delay in endometriosis: a contemporary systematic review. BJOG 2025.
- Rahmioglu N, Mortlock S, Ghiasi M, et al. The genetic basis of endometriosis and comorbidity with other pain and inflammatory conditions. Nat Genet 2023;55:423–436.
Add as a Preferred Source on Google
You can add draksoyivf.com as one of your preferred health information sources on Google.

The content has been created by Dr. Senai Aksoy and medically approved.